This article describes the range of services available for patients with skin disease in the United States. Within the structure of health care systems, 4 levels of care are characterized and discussed: self-care and management, generalist care, specialist care, and subspecialist care. Within each level, this article discusses the profiles of individuals involved in delivering medical care, the location or setting in which these services are provided, the capacity and specific activities of care providers, and current literature on the efficacy of these different levels of care.
The impact of skin disease in the United States is significant and growing. In 2004, skin diseases were 1 of the top 15 groups of medical conditions that experienced the greatest increase in both prevalence and health care spending from 1987 to 2000. Approximately 1 of 3 people in the United States have 1 or more of the 3000 identified skin diseases at any given time. In a joint project by the American Academy of Dermatology (AAD) and the Society for Investigative Dermatology, the total economic burden of skin disease in 2004 was estimated at $96 billion, taking into account the annual cost of skin disease of $39.3 billion (direct medical costs and lost productivity costs) and the additional economic burden of skin disease on quality of life estimated at $56.2 billion.
This article describes the range of services available for patients with skin disease in the United States. Within the structure of health care systems, 4 levels of care are characterized and discussed: self-care and management, generalist care, specialist care, and subspecialist care. Within each level, this article discusses the profiles of individuals involved in delivering medical care, the location or setting in which these services are provided, the capacity and specific activities of care providers, and current literature on the efficacy of these different levels of care.
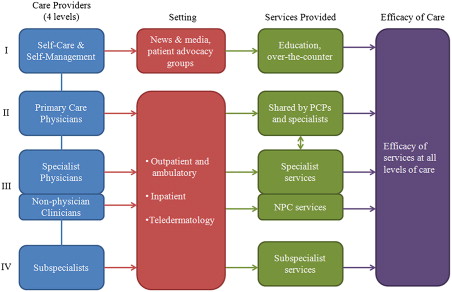
Four levels of health care providers
Level 1: Self-care and Self-management
In the first level of care, self-care refers to individuals’ actions to gain or maintain a level of health, which may be distinguishable from self-management, which refers to an individual’s modification of a management plan that was guided by a clinician at some point.
This level of care is guided mainly by knowledge that is obtained and understood by the individual. Patient education is an essential component of the framework of patient-centered medicine. In this setting, patients are enlisted as partners with the physician in managing their medical condition. With noncompliance becoming a central issue in the treatment of dermatologic conditions, patient knowledge of and participation in the treatment of their disease play a vital role in providing effective care.
Level 2: Primary Care
Primary care refers to care provided by physicians who have received postgraduate training in pediatrics, family or general practice, and internal medicine. Primary care physicians (PCPs) are trained to have fundamental knowledge of common diseases of all organ systems, thus they serve the role to make basic diagnoses and provide nonsurgical treatment of common medical conditions. They often provide the first contact for an undiagnosed health concern, as well as continuing care for most patients.
PCPs provide substantial medical care to patients with dermatologic conditions. From 1990 to 1994, 5% of all outpatient visits to internists and 7% of all visits to family physicians were for dermatologic diseases. In 1998, nondermatologists were estimated to provide care for 56% of visits for common skin complaints, whereas dermatologists managed approximately 40% of outpatient visits for dermatologic problems. Under managed care, which was the dominant mechanism of payment for the treatment of skin disease for many patient groups in the 1990s, primary care providers acted as the gatekeepers, serving as the first point of access to health care for the primary purpose of reducing health care cost and resource use. In 1996, Ramsay and Weary suggested that public opinion still favored the idea of the Marcus Welby physician, a primary care provider capable of providing quality care in all aspects of medicine. However, treatment of skin conditions by dermatologists has been shown to be more cost-effective, because of the superior diagnostic skills of dermatologists in managing skin diseases and the ability of dermatologists to treat skin problems using less physician time. Studies have provided consistent evidence supporting the cost-effectiveness and superior quality of care with direct access to specialists, and gatekeeping has ceased to be the primary mechanism of payment. Studies suggest that public perception has also shifted, and many patients may prefer dermatologic specialists to primary care.
PCPs are now second to dermatologists in providing care for skin conditions. They continue to perform a significant volume of skin-related procedures in the United States, and almost exclusively treat certain skin conditions, such as impetigo. According to data from the National Ambulatory Medical Care Survey (NAMCS), a survey collecting information on outpatient services in the United States, general or family practitioners performed 12% of all dermatologic procedures in 2007 and 11% in 2008, whereas dermatologists performed 60% and 45% of procedures in 2007 and 2008, respectively.
Level 3: Specialists
Specialist care for skin disease is provided by the dermatology workforce in the United States, which includes dermatologists (physicians who have undergone at least 4 years of postgraduate training in the treatment of skin disease) as well as other health care practitioners supervised by dermatologists: nurse practitioners (NPs), physician assistants (PAs), and clinical triage assistants (CTAs). A smaller volume of dermatologic procedures are performed by plastic surgeons, who are specialists with some training in cutaneous surgery.
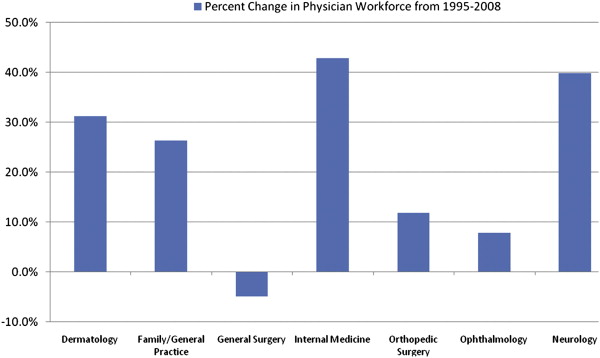
A shortage of physicians in the US dermatology workforce has been documented since 1999, because of a combination of increased demand for services, limited training positions for new physicians, and changes in the demographics and distribution of physicians. In more recent years, with an aging population and increasing prevalence of certain skin diseases such as melanoma and nonmelanoma skin cancer, and with greater access to specialists, the demand for dermatologic services has been increasing. Because of limited training positions for dermatologists in the United States, there has been limited increase of dermatologists compared with other specialties such as internal medicine and neurology ( Fig. 1 ), and the overall size of the dermatology workforce continues to be smaller than other specialties such as orthopedic surgery, ophthalmology, and neurology ( Fig. 2 ). Instead, data indicate a rapid influx of nonphysician clinicians (NPCs) or physician extender clinicians to the dermatology workforce to meet the increasing needs. These NPCs include NPs, physicians’ assistants, and CTAs, who work with dermatologists to provide care.
Related posts:
 A Review of Health Outcomes in Patients with Psoriasis
Health Outcomes in Atopic Dermatitis
Contact Dermatitis in the United States: Epidemiology, Economic Impact, and Workplace Prevention
Nonmelanoma Skin Cancer
Needs Assessment for General Dermatologic Surgery
Needs Assessment for Mohs Micrographic Surgery
A Review of Health Outcomes in Patients with Psoriasis
Health Outcomes in Atopic Dermatitis
Contact Dermatitis in the United States: Epidemiology, Economic Impact, and Workplace Prevention
Nonmelanoma Skin Cancer
Needs Assessment for General Dermatologic Surgery
Needs Assessment for Mohs Micrographic Surgery
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


