Serratus Anterior Flap for Chest Wall Reconstruction
Zachary J. Collier
David H. Song
DEFINITION
Chest wall deformities arising from congenital malformations and acquired etiologies result in significant physical and psychological sequelae.
Regardless of the underlying etiology, failure to reconstruct chest wall deformities may result in debilitating respiratory abnormalities, risk of internal organ injury, and psychological ramifications.
Serratus anterior flap (SAF)
SAF was first described in 1979 by Mathes and Nahai and later refined in 1982 by Takayanagi and Tsukie1 for use as a muscle transposition flap based off of a type III (two major pedicles) vascular supply.
The SAF has been employed as a transposition and free flap for reconstructing defects of the upper and lower limbs, trunk, and head and neck.
It is a highly versatile small to medium-sized muscle flap that can be neurotized through the sensory branches of the intercostal nerves over the skin paddle as well as incorporated into a larger chimeric design for more complex reconstructions.
ANATOMY
The chest wall is a complex musculoskeletal system that provides a rigid skeletal encasement for protecting vital organs while maintaining the flexibility to interact with multilayered and vectored musculature to facilitate respiration and upper extremity mobilization.
The skeletal system is composed of 2 clavicles and 12 paired ribs, which in turn articulate posteriorly with the thoracic vertebrae’s costal facets and transverse processes as well as anteriorly with the sternum via costochondral joints. The 8th to 10th ribs are referred to as “false” ribs as they lack direct sternal attachments, whereas ribs 11 and 12 are termed the “floating” ribs (FIG 1).
The musculature is composed of two main groups—axial and appendicular muscles (FIG 2).
Most axial muscles can be divided into two subtypes based on their role in respiration—inspiratory (sternocleidomastoid and scalene) and expiratory (rectus abdominis, internal oblique, and external oblique)—although the trilayered intercostals participate in both respiratory processes.
The appendicular muscles are required for manipulation of the scapula (trapezius, serratus anterior) and humerus (pectoralis major/minor, latissimus dorsi).
The serratus anterior originates from the superolateral borders of the first 8 or 9 ribs and inserts onto the costal surface of the medial scapular border to create 7 to 10 distinct digitations or slips (average dimension 10 × 20 cm).2
The distribution of serratus digitations is as follows: 7 (13%), 8 (48%), 9 (26%), and 10 (13%).3
Arterial supply (Mathes and Nahai type III)
Superior 3 to 5 slips: The lateral thoracic artery (0.5 to 1.5 mm),4 which originates from the axillary artery posterior to the pectoralis minor, follows the inferolateral border of the muscle to supply the first 3 to 5 slips.
Inferior 3 or 4 slips: The thoracodorsal artery (2 to 4 mm),5 which originates from the subscapular artery, gives off one (40%), two (50%), or three (10%) serratus branches (1.5 to 2.5 mm)6 to supply the inferior 3 to 4 slips. The average pedicle length is 11 cm but may be as long as 15 cm if taken to the subscapular artery.3
Veins: Paired venae comitantes run parallel to their arterial counterparts (FIG 3).
Nerves: Innervated by the long thoracic nerve, which arises from the C5 to C7 anterior rami and passes through the cervicoaxillary canal, it runs posterior to the brachial plexus and axillary artery/vein where it follows the inferior surface of the muscle and eventually diverges on the vascular pedicle as it travels inferiorly.6
Preserve the first 4 or 5 muscular slips to avoid damage to this nerve, which would produce a winged scapula deformity.
Innervation of the optional skin paddle is provided by the lateral cutaneous branches of the intercostal nerves (FIG 4).
PATHOGENESIS
Congenital
Pectus excavatum (PE), pectus carinatum (PC), Poland syndrome, anterior thoracic hypoplasia, pentalogy of Cantrell, asphyxiating thoracic dystrophy, spondylothoracic dysplasia, and sternal clefts
Acquired
Trauma, tumor resections, postoperative complications, wound infections involving musculoskeletal components, and chronic empyemas
PATIENT HISTORY AND PHYSICAL FINDINGS
History
As with any other reconstructive procedure, a thorough evaluation of comorbidities, especially those that place the patient at risk for VTEs (ie, history of VTEs, obesity, diabetes, smoking, Caprini score greater than 8)7 or vascular complications, is critical for preoperative medical and anesthesia optimization.
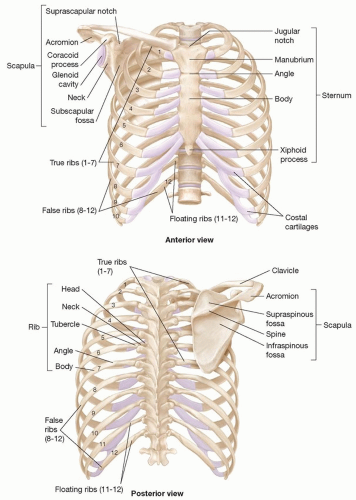
FIG 1 • Skeletal anatomy of the chest wall.
Congenital: It is important to acquire any genetic workup or syndromic diagnoses in order to identify additional comorbidities and underlying structural abnormalities not readily apparent on physical exam that may complicate or alter the surgical approach.
Acquired: History of insults to the chest wall soft tissue and skeletal integrity is critical for identifying the full extent of the defect as well as any factors that may influence the treatment plan.
Trauma: Consider imaging (magnetic resonance imaging [MRI], computed tomography [CT], vascular imaging) studies if there is a potential for aberrant/obscured anatomy or foreign bodies.
Infection: Consider tissue quantifications and cultures to identify any pathologic microbes and to guide preoperative planning regarding plating and/or other hardware utilization.
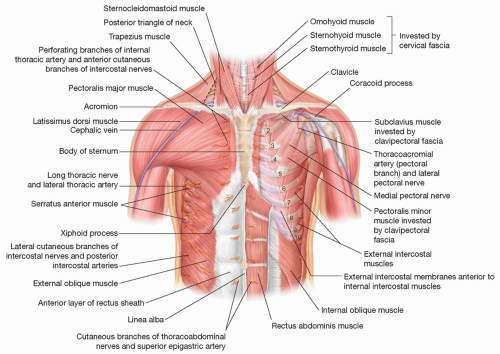
FIG 2 • Musculature and neurovascular anatomy of the chest wall.
Oncologic: Ensure clear pathologic margins or identify additional resection requirements and treatment goals respective to tumor type.
Radiation: Identify plans for postadjuvant radiation therapy to guide reconstructive decisions (ie, local/regional vs free flap design, timing).
Physical exam
In general, identification of defect dimensions and involved tissue types is critical for preoperative planning and flap design.
Skin: Note scars or contractures from prior procedures. Identify lacerations for potential utilization as or integration with incision design. Evaluate for skin integrity including turgor, elasticity, and signs of radiation damage or dermatologic disease.Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree