Clinical type
Skin manifestations
Basically match those of adolescent/adult AD:
Chronic eczema on the face and neck and exudative/lichenified eczematous dermatitis on the trunk and extremities
Other stigmas of AD, e.g., atopic red face, Hertoghe’s sign, Dennie-Morgan’s infraorbital folds, dirty neck, etc., are observed
Features of elderly AD that differ from adolescent/adult AD:
The classic sign of localized lichenified eczema in the folds of the elbows and knees is uncommon
Unaffected folds of the elbows and knees are common
IgE reactivity and cytokines
Major allergens for IgE-allergic elderly AD: HDMs (Dermatophagoides species) followed by pollens [4, 12]
Dominance of Th2 cytokine profiles, i.e., IL-4, IL-5, and IL-13 in elderly patients with IgE-allergic elderly AD [4]
Dominance of Th1 cytokine profiles, i.e., IL-2 and IFN-γ in elderly patients with low serum total IgE [4]
Histopathology and immunopathogenesis of skin lesions
Numerous IgE+ cells, i.e., MCs, CD11c+ inflammatory DCs, and CD1a+ epidermal DCs are found among inflammatory cells infiltrating in IgE-allergic elderly AD [22, 33]
Existence of HDM allergens coincident with IgE+ DCs can be observed in the skin lesions of elderly patients with IgE-allergic AD and HDM sensitization [33]
Only a few IgE+ MCs are found among inflammatory cells infiltrating in non-IgE-allergic elderly AD [22]
Diagnosis of elderly AD
A long follow-up (more than 6 months), analyses of diagnostic features of AD, and exclusion from other pruritic skin conditions are required
Epidemiology
The prevalence of elderly AD is approximately 1–3% among elderly individuals in industrialized countries [4, 43]
Onset and clinical course
Personal and family histories of disorders associated with AD
Associations with clinical phenotypes and asthmatic complications are seen in elderly patients with IgE-allergic AD with onset before 30 years old [12]
Lower incidence of ichthyosis in elderly patients with IgE-allergic AD [12]
Complications of coexisting/underlying disorders and malignancy
Most elderly AD patients have some complications of nonallergic coexisting/underlying disorders
Management and prognosis
Majority of elderly AD patients show good prognosis after suitable management
Powerful anti-inflammatory treatments like oral corticosteroids may be needed in moderate to severe cases
Complete remission (outgrowth) rarely arises
Most elderly AD patients reach the end of life with AD [12]
18.2.1 Clinical Type
In general, at least two types of AD have been identified: an immunoglobulin (Ig)E-allergic type associated with high levels of serum total IgE (more than approximately 200 or 400 IU/L, according to the standards of the individual facility) and IgE-mediated sensitization to environmental allergens (positive results of allergen-specific IgE in skin prick test and/or serum evaluations) and a non-IgE-allergic type with normal levels of serum total IgE and a lack of sensitization to environmental allergens [9, 10]. Similar to other age groups, both IgE-allergic and non-IgE-allergic types of AD exist in elderly AD, if the diagnosis of AD is based upon standardized diagnostic criteria [6]. In addition, as is the case with infantile AD [11], an indeterminate-allergic type also exists in elderly AD with normal levels of serum total IgE and positivity for allergen-specific IgEs or with high levels of serum total IgE and non-detectable allergen-specific IgEs, as an intermediate, vague state between IgE-allergic and non-IgE-allergic types. In our clinical study (n = 60), the frequencies of IgE-allergic type, indeterminate-allergic type, and non-IgE-allergic type in elderly AD were 63.3% (n = 38), 15.0% (n = 9), and 21.7% (n = 13), respectively [12].
18.2.2 Skin Manifestations
The characteristics of skin manifestations seen in elderly AD basically match those of adolescent/adult AD [2]. Chronic eczema on the face and neck and exudative/lichenified eczematous dermatitis on the trunk and extremities are observed as major symptoms in elderly AD. Other stigmata of AD such as refractory facial erythema (atopic red face), Hertoghe’s sign (loss of the lateral eyebrows), Dennie-Morgan’s infraorbital folds, and dirty neck are observed mainly in moderate to severe cases (Fig. 18.1a–f). Nummular-form eczema, prurigo-form papules and/or nodules, chronic hand and/or foot eczema, and erythrodermic rash may also be observed (Fig. 18.1g–k).


Fig. 18.1
Skin manifestations of elderly atopic dermatitis. (a) Lichenified eczema with post-inflammatory depigmentation, Hertoghe’s sign (loss of lateral eyebrows), and Dennie-Morgan’s infraorbital folds on the face. (b) Refractory eczematous erythema (atopic red face) on the face. Figure reproduced with permission from the Japanese Journal of Allergology [7]. (c) Lichenified eczema on the neck and upper back. Figure reproduced with permission from Geriatrics & Gerontology International [8]. (d) Lichenified eczema with post-inflammatory depigmentation on the neck (dirty neck). (e) Eczematous dermatitis with a diffuse exudative inflammation on the trunk. (f) Diffuse lichenified eczema on the trunk and localized lichenified eczema in the right elbow fold. (g) Nummular-form eczema on the back. (h) Prurigo-form papules on the left arm. (i) Lichenified hand eczema. (j) Lichenified foot eczema. (k) Lichenified eczema of erythroderma on the trunk
One feature of skin manifestations in elderly AD that might distinguish this form from adolescent/adult AD is the involvement of the folds of the elbows and knees. Localized lichenified eczema in the elbow and knee folds is a typical sign of classic childhood AD and adolescent/young adult AD [1, 5, 17], but is uncommon in elderly AD [3, 12]. In elderly AD, unaffected folds of the elbows and knees are common, and lichenified eczema surrounding the folds, particularly around the elbow folds, are frequently observed. In our clinical study of 38 patients with IgE-allergic elderly AD [12], lichenified eczema in the flexure and/or extensor sites of the upper and lower extremities were observed in 30 patients (78.9%) and 22 patients (57.9%), respectively. However, a lack of lichenified eczema in the folds of elbows and knees was observed in 29 patients (76.3%) and 28 patients (73.7%), respectively. The classic sign of localized lichenification in the elbow and knee folds was observed in only two patients (5.3%) and four patients (10.5%), respectively (Fig. 18.2a, d). Diffuse lichenified eczema in the flexure sites of the extremities, including the elbow and knee folds, was observed in seven patients (18.4%) and six patients (15.8%), respectively (Fig. 18.2b, e). On the other hand, the reverse sign of lichenified eczema around unaffected folds of the elbows and knees was observed in 15 patients (39.5%) and in 5 patients (13.2%), respectively (Fig. 18.2c, f). This feature of scarce involvement in the folds of the elbows and knees in elderly AD might be partly associated with age-related decrements in regional sweat function [8, 13], because sweating can be related to the development of skin lesions of AD at these sites [14], and a pathophysiology of AD as an irritant, a major source of skin moisture, and an allergen for immediate hypersensitivity reactions [14–16].
Fig. 18.2
Lichenification (lichenified eczema) in the antecubital and popliteal areas of elderly patients with atopic dermatitis. (a) Localized lichenified eczema in the elbow fold. (b) Diffuse lichenified eczema in the elbow fold and flexure site of the arm. (c) Lichenified eczema around the scarcely involved elbow fold. Figures reproduced with permission from the Journal of Clinical Medicine [12]. (d) Localized lichenified eczema in the knee fold. (e) Diffuse lichenified eczema in the knee folds and flexure site of the lower extremities. (f) Lichenified eczema around the scarcely involved knee fold
18.2.3 IgE Reactivity and Cytokines
The average level of serum total IgE in elderly patients with IgE-allergic AD has been reported as 2540 ± 2234 IU/mL in Poland [4] and 6975 ± 9908 IU/mL according to a previous study in our hospital [12]. The most common environmental allergens for IgE-allergic elderly AD are house dust mites (HDMs; e.g., Dermatophagoides species), followed by pollens (e.g., grass pollen and Japanese cedar). Positive rates were as follows: D. pteronyssinus (Der p), 72%; D. farinae (Der f), 70.9%; and grass pollen, 68.4% in the Polish study [4], and Der f, 83.8%, and Japanese cedar, 56.8% in the study of our patients [12]. Positive rates for foods, fungus, and animal dander were relatively lower in those studies. Der f also showed the highest average of titers for specific IgEs to environmental allergens in our patients [12].
Phenotypic analyses of peripheral blood cytokine concentrations in the Polish study [4] demonstrated the dominance of a T-helper (Th)2 cytokine profile, i.e., interleukin (IL)-4, IL-5, and IL-13, in elderly patients with IgE-allergic AD, and dominance of a Th1 cytokine profile, i.e., IL-2 and interferon-γ, in elderly patients with AD and low serum total IgE.
18.2.4 Histopathology and Immunopathogenesis of Skin Lesions
The pathogenesis of AD is complex. Recent research has provided a new concept for the immune pathomechanisms underlying AD, assigning roles to innate and adaptive immunity associated with Th1, Th2, Th17, Th22, and T-regulatory cells as well as innate lymphoid cells, macrophages, dendritic cells (DCs), mast cells (MCs), eosinophils, basophils, and keratinocytes [17–21].
On histopathological analysis, a chronic eczematous reaction with inflammatory infiltrating cells, mainly comprising cluster of differentiation (CD)4+ and CD8+ T cells, MCs, macrophages, and eosinophils, is observed in the lichenified eczema of elderly AD [22]. The composition of infiltrating cells is broadly the same as the compositions of nonatopic chronic dermatitides (e.g., asteatotic dermatitis), except for the increase in MCs [3, 22].
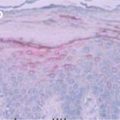
Among elderly patients with IgE-allergic AD, IgE-mediated allergic inflammation plays a critical role in the features of skin lesions. Immunohistochemical analysis of our previous study [22] showed IgE+ MCs in the upper dermis (Fig. 18.3a, b), IgE+ CD11c+ DCs (myeloid DCs; so-called atopic DCs [23]) in both the epidermis and upper dermis (Fig. 18.3c), and IgE+ CD1a+ DCs (myeloid DCs; mostly Langerhans cells [24]) in the epidermis in the lichenified eczema of IgE-allergic elderly AD. IgE+ CD11c+ DCs are a type of inflammatory DC, and a group of IgE+ CD11c+ DCs with “CD1a+” could be termed as inflammatory dendritic epidermal cells when they infiltrate into the epidermis [17, 23, 25]. In contrast, although just a few IgE+ MCs were detected, no IgE+ CD11c+ cells or IgE+ CD1a+ cells were found in the lichenified eczema of non-IgE-allergic AD (Fig. 18.3d–f). As with the clinical condition of atopic allergy, immune histopathology of indeterminate-allergic AD showed a vague state between IgE-allergic and non-IgE-allergic AD. In control cases, only a few IgE+ MCs were observed in asteatotic dermatitis (Fig. 18.3g–i). In addition, although moderate IgE+ MCs and slight IgE+ CD1a+ DCs were observed, no IgE+ CD11c+ cells were found in the epidermis or upper dermis in noneczematous disorders with elevated serum total IgE levels (e.g., cholesterol embolism and Churg-Strauss syndrome) (Fig. 18.3j–l).
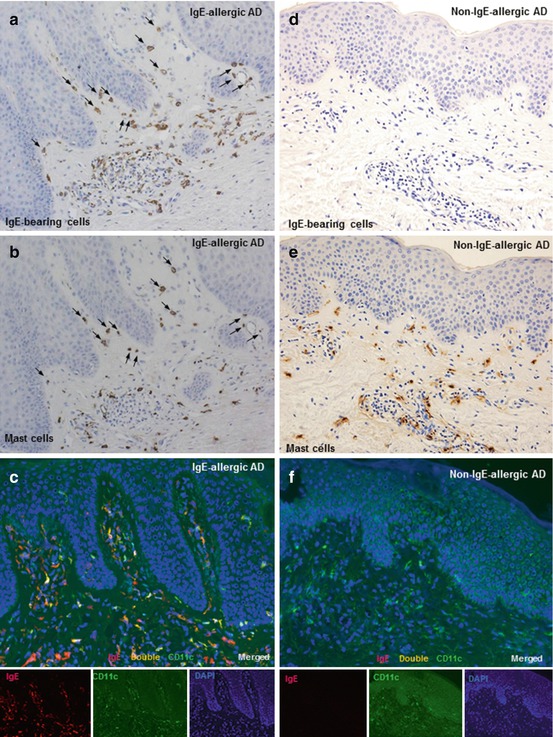
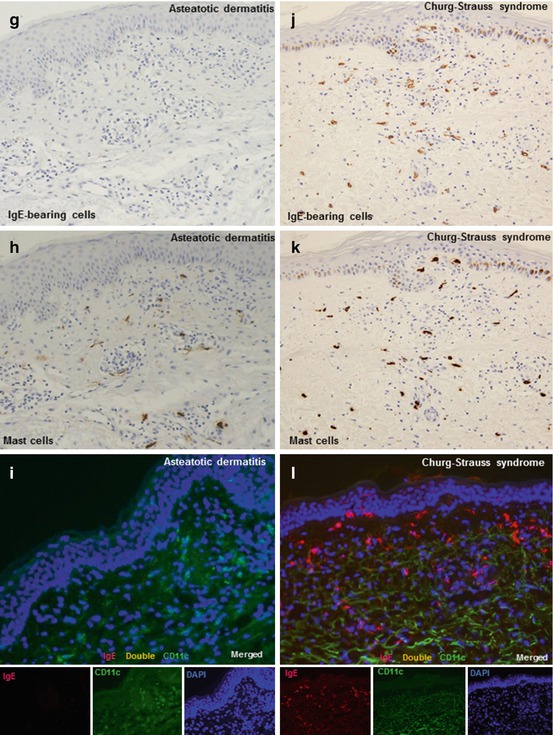
Fig. 18.3
Single immunohistochemical and double immunofluorescence staining with anti-immunoglobulin (Ig)E, anti-mast cell tryptase, and anti-cluster of differentiation (CD)11c monoclonal antibodies [22]. A lichenified skin lesion from an elderly patient with IgE-allergic atopic dermatitis (AD): (a–c). (a) Numerous IgE+ cells are seen in inflammatory infiltrating cells in the upper dermis. Original magnification: ×100. (b) Tryptase + mast cell infiltration is increased in the upper dermis. Original magnification: ×100. Note that, in (a) and (b), the majority of IgE+ cells and tryptase + mast cells in the upper dermis show the same morphology and localization (arrows). (c) Double-positive IgE+ CD11c+ cells (yellow images) accompanied by single-positive IgE+ cells (red images) and single-positive CD11c+ cells (green images) are observed in the epidermis and upper dermis. Original magnification: ×200. Figures reproduced with permission from the Journal of the European Academy of Dermatology and Venereology [22] and the Japanese Journal of Allergology [7]. A lichenified skin lesion from an elderly patient with non-IgE-allergic AD: (d–f). (d) Few IgE+ cells are present in inflammatory infiltrating cells in the upper dermis. Original magnification: ×100. (e) Tryptase + mast cell infiltration is increased in the upper dermis. Original magnification: ×100. (f) Only single CD11c+ cells (green images) are observed in the epidermis and upper dermis. Original magnification: ×200. Figures reproduced with permission from the Japanese Journal of Allergology [7]. An eczematous skin lesion from an elderly patient with nonatopic chronic eczema (asteatotic dermatitis): (g–i). (g) Few IgE+ cells are present in inflammatory infiltrating cells in the upper dermis. Original magnification: ×100. (h) Tryptase + mast cells are observed in the upper dermis. Original magnification: ×100. (i) Only single-positive CD11c+ cells (green images) are apparent in the upper dermis. Original magnification: ×200. Figures reproduced with permission from the Journal of the European Academy of Dermatology and Venereology [22] and the Japanese Journal of Allergology [7]. A skin lesion of vasculitis from an elderly patient with Churg-Strauss syndrome: (j–l). (j) Numerous IgE+ cells are observed in inflammatory infiltrating cells in the upper dermis. Original magnification: ×100. (k) Tryptase + mast cell infiltration is seen in the upper dermis. Original magnification: ×100. Note that, in specimens of (j) and (k), most IgE+ cells and tryptase + mast cells in the upper dermis show the same morphology and localization. (l) The majority of infiltrating stained cells in the epidermis and upper dermis represent single IgE+ cells (red images). No double-positive IgE+ CD11c+ cells (yellow images) are observed. Original magnification: ×200. Figures reproduced with permission from the Japanese Journal of Allergology [7]. Single immunohistochemical staining using serial paraffin sections (a, b, d, e, g, h, j, and k) and double immunofluorescence staining using frozen sections (c, f, i, and l). In the immunohistochemical staining, sets of figures (a and b, d and e, g and h, and j and k) represent serial sections. In the immunofluorescence staining, nuclei are labeled with 4′,6-diamidino-2-phenylindole (DAPI, blue images). Clinical findings: IgE-allergic AD, a 71-year-old man with an elevated serum total IgE level of 2413 IU/mL and specific IgEs for Dermatophagoides farinae (Der f) and Japanese cedar; non-IgE-allergic AD, a 63-year-old man with a serum total IgE level of 42 IU/mL and no detectable specific IgEs; asteatotic dermatitis, an 86-year-old man with a serum total IgE level of 16 IU/mL and no detectable specific IgEs; and Churg-Strauss syndrome, a 78-year-old man with an elevated serum total IgE level of 3007 IU/mL and weak positivity for specific IgEs for Der f
Complexes of IgE and high-affinity receptor (Fc epsilon receptor type I) on the cell surface of IgE+ MCs, IgE+ CD1a+ DCs, and IgE+ CD11c+ DCs can capture a large amounts of allergens [17, 22, 23], and IgE+ MCs may induce IgE-mediated immediate- and late-phase hypersensitivity reactions [26, 27], and the IgE+ CD1a+ DCs and IgE+ CD11c+ DCs might cause IgE-associated delayed-type hypersensitivity reactions as a result of the efficient presentation of allergens to naïve and/or specific memory T cells [28–30]. The possibility of eczematous skin reactions induced only by IgE-allergic sensitization has been reported using murine models [26]. The existence of HDM allergens in the dermis and epidermis coincident with DCs in naturally occurring AD lesions [31] and with IgE+ DCs in the site of atopy patch test for HDM [32] has been reported in adult patients with IgE-allergic AD and HDM sensitization. Indeed, the existence of HDM allergens (e.g., Der f 1) coincident with IgE+ CD11c+DCs (e.g., CD207+ Langerhans cells) in the upper dermis (Fig. 18.4a, b) and with IgE+ CD1a+ DCs (e.g., CD207+ Langerhans cells) in the epidermis (Fig. 18.5a–d) could be observed in the lichenified eczema of elderly patients with IgE-allergic AD and HDM sensitization in our immunohistological studies [33]. These findings suggest that not only IgE-mediated immediate- and late-phase hypersensitivities but also IgE-associated delayed-type hypersensitivity might contribute to the immunopathogenesis of skin manifestations of IgE-allergic elderly AD.
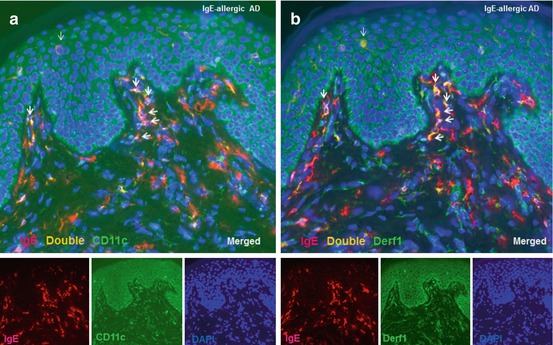
Fig. 18.4




Double immunofluorescence staining with anti-immunoglobulin (Ig)E and anti-cluster-of-differentiation (CD)11c monoclonal antibodies and anti-Dermatophagoides-farinae (Der f) 1 polyclonal antibodies. Figures (a and b) represent serial sections. (a) Double-positive IgE+ CD11c+ cells (yellow images) are observed in the upper dermis of lichenified eczema of an elderly patient with IgE-allergic atopic dermatitis (AD). Original magnification: ×200. (b) Double-positive IgE+ Der f1+ cells (yellow images) are also observed in the upper dermis of lichenified eczema. Original magnification: ×200. Note that, in specimens of (a) and (b), the majority of IgE+ CD11c+ cells and IgE+ Der f1+ cells in the papillary dermis show the same morphology and localization (thick arrows). However, coincidental presence of an IgE+ CD11c− cell and an IgE+ Der f1+ cell in the epidermis is also observed (thin arrows). Figures reproduced with permission from the Dermatology Clinics & Research [33]. Clinical findings: IgE-allergic AD, an 84-year-old man with an elevated serum total IgE level of 19,757 IU/mL and specific IgEs for Dermatophagoides farinae and other environmental allergens
Related posts:

Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
