Abstract
Liposuction was designed to correct unaesthetic deposits of subcutaneous fat; it produces satisfactory silhouette contouring when performed by appropriately trained plastic surgeons using properly selected technologies. However, from lipoaspirate it is possible to obtain autologous fat graft and adipose-derived stem cells (ADSCs) for reconstructive surgery and regenerative medicine. Autologous fat transplantation uses include the correction of body contour, malformations, and post-surgical outcomes. The aim of this chapter is to highlight the crucial role of adipose tissue in plastic and reconstructive surgery, from liposuction to lipofilling and ADSCs, exposing the indications, procedures, and complications of these surgical techniques. The Stromal Enriched Lipograft (SEL) is a new surgical technique of autologous fat grafting for body contouring which converts a stem cell poor fat graft to a stem cell rich fat graft. The clinical outcomes of scientific research in the last decade have shown that SEL is one of the core elements of regenerative medicine.
7 The Role of Stem Cells in Body Contouring
Key Points
In this chapter, the technique, pearls, and pitfalls of SEL are described in detail. A series of patients who underwent contouring of abdomen and trunk assisted by SEL are presented.
Careful selection of patients and proper surgical technique help avoid contour irregularity, and outcome expectations should be based on realistic preoperative evaluation of the patient’s age, skin elasticity, volume of fat to be removed, and volume of fat to be transplanted.
SEL technique aims at filling preoperatively marked deficiencies with adipocytes and adipose-derived stem cells that will survive and become incorporated into the recipient bed.
Improvement of the gluteal contour and body contour can be attained and maintained through autologous fat transplantation by means of SEL.
Irregularities ranging from “over suctioning” to bumpy skin and asymmetries result from an overaggressive approach to liposuction of the flanks and SEL technique can play a significant role in repairing such iatrogenic defects.
7.1 Introduction
The improvement of surgical techniques in autologous fat transplantation has increased the survival rate of the grafted fat and has reduced the side effects such as fat necrosis. Several mechanisms may contribute to the variability of outcomes for fat-grafting procedures. The harvesting process is traumatic to adipocytes, which can lead to apoptosis. Additionally, results for recipient wound beds with different degrees of blood supply and fluctuations in oxygen delivery may range from adequate revascularization and good “take” to insufficient revascularization and ischemia, apoptosis, and dedifferentiation of central adipocytes. 1 A significant proportion of the engrafted fat undergoes resorption and necrosis due to the non-vascularized nature of the transplant. Resorption rates after fat grafting are generally reported to be between 20 and 80%. 2 Therefore, in order to maximize survival, multiple passes in different tissue planes are required in order to optimize plasmatic imbibition and neovascularization of the transplanted fat grafts. Injection of the fat graft should be met with minimal resistance and a small volume is administered upon entry with the remaining volume given during withdrawal to minimize trauma. Adipose tissue is composed of mature adipocytes constituting about 90% of the tissue volume, and a stromal vascular fraction (SVF) including fibroblasts, endothelial cells, preadipocytes, vascular smooth muscle cells, lymphocytes, resident monocytes/macrophages. It has become apparent over the years that white adipose tissue (WAT) is the most suitable autologous injectable filler for correcting soft tissue defects. 3 Adipose tissue is considered as a source of mesenchymal stem cells (MSCs), termed adipose-derived stem cells (ADSCs). They are ubiquitous and easily obtained in large quantities with little donor site morbidity or patient discomfort making the use of autologous ADSCs an appropriate cellular therapy. The use of ASCs may enhance angiogenesis, improve the survival of grafts, and thus reduce atrophy of the fat grafting. 4 ADSCs have been evaluated in clinical studies for soft tissue augmentation and represent a novel approach to cell-based therapies, such as autologous fat transplantation. Nowadays, autologous fat transplantation or adipose cell grafting incorporates adipocytes, ADSCs and growth factors already present in the lipoaspirate. The SEL is a new surgical technique of autologous fat grafting for body contouring which converts a stem cell poor fat graft to a stem cell rich fat graft. 5 The clinical outcomes of scientific research in the last decade have shown that SEL is one of the core elements of regenerative medicine.
7.2 Patient Selection
Body contouring of the trunk and extremities combines liposuction, excisional surgical techniques, and autologous fat grafting. 6 Body contouring patients should be carefully evaluated for their expectations and the actual results that can be achieved by this procedure. Planning the procedure and indicating it properly is just as important as the surgical procedure itself. Patients who clearly have any psychiatric disorder, such as body dysmorphic disorder are referred for psychiatric evaluation. However there are subtle cases in which patients present low self-esteem, borderline type of anxiety, and unrealistic expectations. In those cases, sometimes it is better to deny operating on the patient. The ideal patient for body contouring procedures has a small amount of adipose tissue to be suctioned out in order to improve the body contour, has small skin laxity, and is dedicated to a healthy lifestyle, including daily physical exercise and a healthy diet. It is the responsibility of the surgeon to address all concerns, risks, goals and expectations of the procedure chosen for the patient in order to avoid false expectations and future frustrations. In this chapter we will address special attention to trunk and thighs including the following areas: upper and lower abdomen, upper and lower back, flanks, pubis and sacrum V-zone, gluteal area, inner thighs, outer thighs, inner knees, and banana rolls.
7.3 Technique
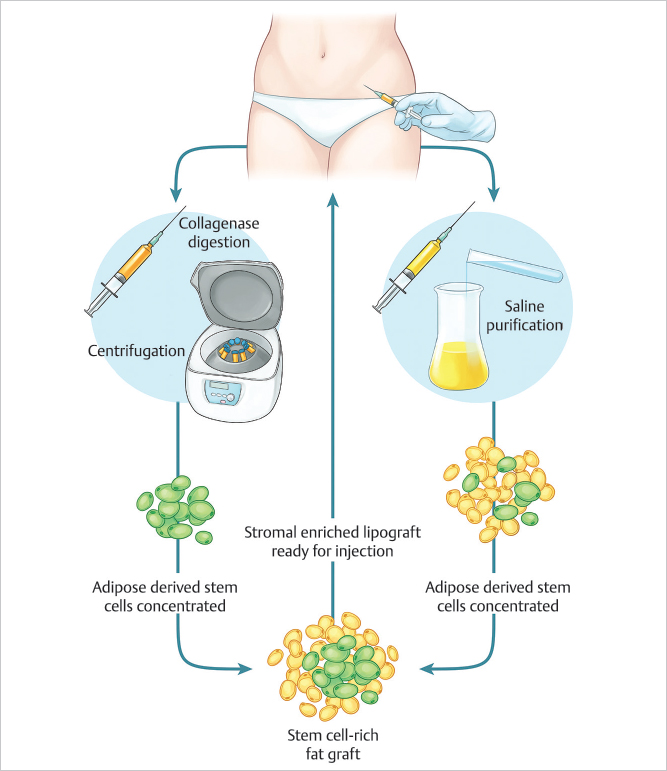
Marking of the areas to be liposuctioned are made while the patient is in standing position. Preoperative sedation in the surgical suite is administered. Anesthesia consists of an epidural block and intravenous sedation. The patient is placed in prone position. After the injection of normal saline wetting solution containing 1:500,000 of adrenaline by a small-bore cannula and waiting 15 minutes, a 60-cc syringe attached to a 4 mm blunt cannula is inserted through small incisions. Fat is aspirated by using the syringe method. The 2/3 of the aspirated fat is used in order to isolate the SVF. Digestion is done with 0.075% collagenase (Sigma, St. Louis, MO) in buffered saline and agitated for 30 minutes at 37°C in Celltibator (Medikan, Los Angeles, CA). Separation of the SVF containing ADSCs is then done by using centrifugation at 1200 × g for 5 minutes. The Lipokit Centrifuge (Medikan, Los Angeles, CA), is used. The SVF is located in the pellet derived from the centrifuged fat at the bottom of the lipoaspirate. In SEL, freshly isolated SVF is attached to the aspirated fat, with the fat tissue acting as a living bioscaffold before transplantation. 7 The remaining 1/3 of the aspirated fat is treated in the following manner: with the syringe held vertically with the open end down, the fat and fluid are separated. Isotonic saline is added to the syringe, the fat and saline are separated and the exudate discarded. The procedure is repeated until the fat becomes yellow in color, free of blood and other contaminants. 8 Mixing of the SVF containing ADSCs and the purified fat is then done (▶Fig. 7.1). This whole procedure is done inside the operating theatre, by 2 tissue engineers, manually, and the time required is about 90 minutes. Tissue planes are created by using specific cannulas in different trajectories, always from the deeper aspect to more superficial areas. Successful fat application is performed using a blunt cannula that creates a tunnel at insertion and the fat is injected as the cannula is withdrawn in order to avoid intravascular fat injection. Multiple passes are used to fan across the deficient region. Antibiotics, analgesics, and anti-inflammatory medications are prescribed during the following 7 postoperative days.
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


