Second Toe to Thumb Transfer
John R. Lien
Kevin C. Chung
DEFINITION
The thumb is critical for hand function.
Toe to thumb transfer is a composite tissue microsurgical reconstructive option for patients with loss of significant thumb length.
ANATOMY
Great toe
Wider pulp and nail plate than native thumb and lesser toes; “thumblike” appearance
Significant aesthetic and functional morbidity at donor site; difficulty with push-off during gait
Second toe
Pulp is bulbous and more rectangular in appearance than the native thumb or fingers.
Interphalangeal joints tend to claw.
Superior cosmetic and functional results on donor foot
Arterial anatomy of the foot
The anterior tibial artery becomes the dorsalis pedis artery (DPA) distal to the ankle extensor retinaculum. The DPA courses along the dorsal foot lateral to the extensor hallucis longus tendon.
At the first intermetatarsal space, the DPA terminally divides into the first dorsal metatarsal artery (FDMA) and the deep plantar artery. The deep plantar artery communicates with the deep plantar arch of the foot, connecting the dorsal and plantar arches (FIG 1).
The FDMA generally travels deep to the extensor hallucis brevis tendon and usually dorsal to the first dorsal interosseous muscle. It then communicates (through the distal communicating artery) with the first plantar metatarsal artery (FPMA) distal to the deep intermetatarsal ligament. The FDMA also terminally branches into the lateral dorsal digital artery of the great toe and medial dorsal digital artery of the second toe, which are of small caliber and clinically insignificant1 (see FIG 1).
FIG 2 shows variants of FDMA anatomy in relation to the first dorsal interosseous muscle, as well as a variant unfavorable for vascular anastomosis.
The plantar digital arteries are the effective blood source to the great and second toes. Their origin is the distal communicating artery connecting the FDMA and FPDA distally (FIG 3).
Venous anatomy of foot
The superficial dorsal venous system is utilized for venous anastomosis.
The dorsal veins of the toes join the dorsal venous arch in the forefoot, which supplies the greater and lesser saphenous veins.
Sensory nerve anatomy of foot
The superficial peroneal nerve innervates the dorsal foot while the deep peroneal nerve innervates the first dorsal web space.
Branches from the posterior tibial nerve innervate the plantar foot and toe pulps. Coaptation of plantar digital nerves are important for pulp sensation.
PATIENT HISTORY AND PHYSICAL FINDINGS
Advanced age is not a contraindication to surgery, but the patient must be in generally good health to tolerate a prolonged surgery.
Active nicotine use and a history of atherosclerotic disease are contraindications to toe transfer.
Assess whether there is adequate, supple skin coverage. If not, consider a staged procedure (groin flap) to increase pliable tissue at the recipient site. Harvesting too much soft tissue from the foot will lead to foot deformity and marked donor-site morbidity.
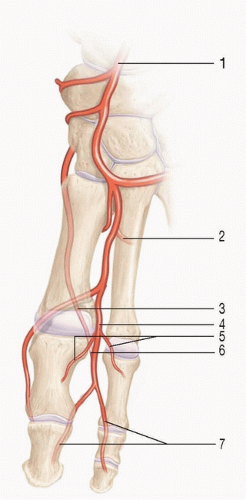
FIG 1 • Dorsal foot arterial anatomy: (1) dorsalis pedis artery (DPA), (2) deep plantar artery, (3) first plantar metatarsal artery (FPMA), (4) first dorsal metatarsal artery (FDMA), (5) dorsal digital arteries, (6) distal communicating branch (intersection of the FDMA and FPMA), (7) plantar digital arteries.
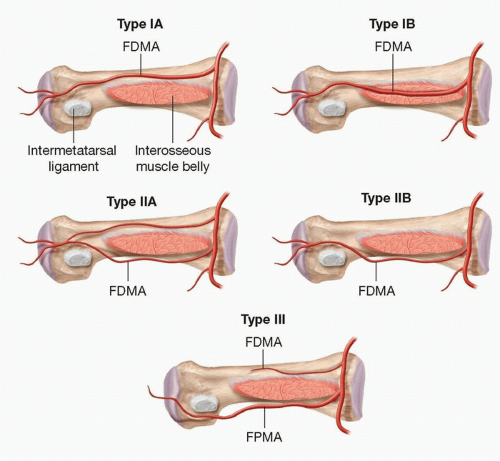
FIG 2 • Variants of first dorsal metatarsal artery (FDMA) anatomy. In type I, the FDMA passes superficial (IA) or within (IA) the interosseous muscle belly. In type II, the FDMA passes at the deep aspect of the interosseous muscle belly but superficial to the intermetatarsal ligament. Type IIA includes a fine accessory branch superficial to the interosseous muscle, whereas IIB does not have an accessory branch. In type III, the FDMA is miniscule or absent with plantar-dominant (FPMA) flow.
The level of thumb amputation will dictate harvest length.
Assess the donor foot (contralateral foot for second toe transfer) to ensure no prior trauma or surgery that would alter vascular anatomy to the second toe. Doppler ultrasound examination can be used to confirm presence of DPA and FDMA.
IMAGING
Review preoperative radiographs of the recipient site to prepare for bone fixation and length requirement of donor toe (FIG 4).
We do not routinely obtain preoperative angiography of the foot, but this is an option if there is concern for altered vascular anatomy on physical and Doppler exam.
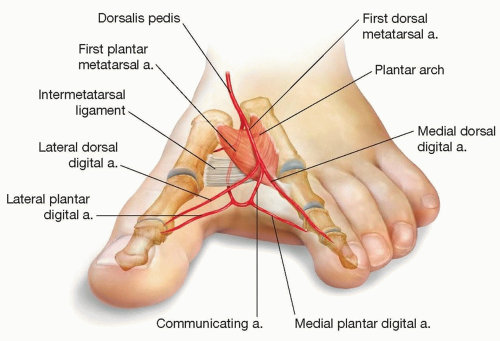 FIG 3 • First web space arterial anatomy. |
SURGICAL MANAGEMENT
Toe to thumb transfer is generally performed after the acute traumatic injury has healed and adequate soft tissue coverage is obtained.
Ensure adequate soft tissue coverage and pliability prior to transfer.
Amputations through the thumb metacarpal (with preserved carpometacarpal joint) or proximal half of the proximal phalanx are good candidates for toe transfer. We prefer the second toe transfer to minimize donor-site morbidity. Other options for toe transfer include great toe and trimmed great toe. Alternatives to toe transfer include metacarpal bone lengthening and on-top plasty. Osteoplastic reconstruction of the thumb using iliac crest bone graft and groin flap is of historical significance only.
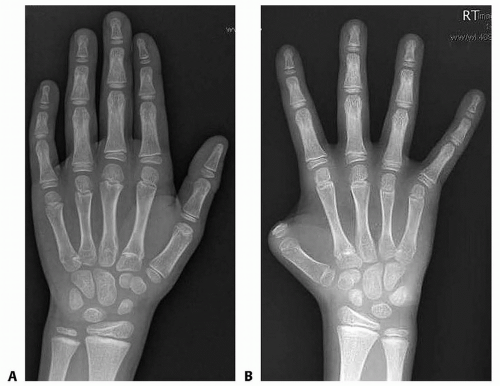
FIG 4 • Preoperative radiograph of recipient hand. Amputation level is at the proximal phalanx base. Contralateral radiographs help estimate defect length.
Amputations at the distal proximal phalanx or distal phalanx often retain enough length for thumb function. Web space deepening may be performed as needed.
Amputations through the base of the metacarpal or though the carpometacarpal joint require index finger pollicization to recreate a basilar thumb joint.
Preoperative Planning
The contralateral toe vascular pedicle is in a better position for radial artery anastomosis at the snuffbox.
The length of the transferred toe should be based on the length of the contralateral uninjured thumb (see FIG 4).Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree