Second Toe-to-Thumb Transfer for Hypoplastic Thumb
Amir H. Taghinia
Brian I. Labow
Joseph Upton
DEFINITION
Toe-to-thumb transfer for congenital conditions is usually indicated in cases in which the carpometacarpal joint and (at least) the proximal part of the metacarpal are intact and functional but the remainder of the thumb is absent or diseased.1
Either the great toe or the second toe is typically used for thumb reconstruction. Although the modified great toe looks more like a thumb, the length of first metatarsal that can be harvested without functional loss in the foot is quite limited.
In congenital patients,2 toe-to-thumb transfer is most commonly performed for amniotic constriction bands, symbrachydactyly (atypical cleft hand), transverse failure of formation, (typical) cleft hand, and highly select cases of type IIIB thumb hypoplasia.
The congenital conditions in which the thumb is diseased include macrodactyly and vascular anomalies.
ANATOMY
The second toe is smaller than the normal thumb. It has a lower width to pulp depth ratio, thus appearing more clubbed and bulbous. It has three phalanges and a metatarsophalangeal joint, which, in the foot, functions as a hyperextension joint rather than a flexion joint as in the thumb.
The arterial anatomy of the second toe can be variable. The dorsalis pedis artery is the main proximal blood supply. It gives rise to the first dorsal metatarsal artery (FDMA) and the first plantar metatarsal artery (FPMA) via anastomosis with the medial plantar artery, a branch of the posterior tibial arterial system of the foot.
The FDMA lies superficial to the first dorsal interosseous muscle.

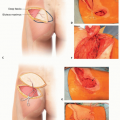
FIG 1 • Variations in arterial anatomy of the first web space of the foot. As it reaches the base of the first and second metatarsals, the dorsalis pedis artery can continue on dorsally as the first dorsal metatarsal artery (FDMA) and send a plantar branch, the first plantar metatarsal artery (FPMA). A. The FDMA may be the dominant blood supply to the second toe and may lie superficially to the first dorsal interosseous. B. Alternatively, the FDMA may lie within or deep to the first dorsal interosseous. C. Last, the FDMA may be diminutive or completely absent.
The FDMA lies within or deep to the first dorsal interosseous muscle.
The FDMA is diminutive or absent.
The more plantar the dominant system, the more difficult is the dissection.
The venous anatomy provides abundant large veins. Venous branches of the second toe reside in the dorsal subcutaneous plane; a vein on either side of the toe drains to the lesser saphenous (lateral) or great saphenous (medial) veins.
The second toe has two extensor tendons—extensor digitorum longus and brevis—and two flexor tendons—flexor digitorum longus and brevis. The extensors approach the second ray in an oblique fashion, from lateral to medial. Two plantar digital nerves travel below the transverse metatarsal ligament and arrive on either side of the toe to provide sensation to the pulp.
Unlike the first ray of the foot where the metatarsal is crucial for gait, the second ray’s metatarsal is expendable and its entire length may be harvested if needed. The goal should be to construct a new thumb of normal length. In full adduction, a normal thumb extends to the proximal interphalangeal (PIP) joint of the adjacent index finger.
In congenital conditions where the foot is also affected, the surgeon may carefully consider harvesting an anatomically abnormal toe. Investigation of arterial anatomy under these special circumstances is, at a minimum, important to avoid vascular compromise of the toe transfer—or worse, the other toes.
In cases of amniotic constriction bands, the proximal anatomy of the hand is usually normal. However, in other conditions such as symbrachydactyly or transverse failure, the anatomy of the hand may not be normal.
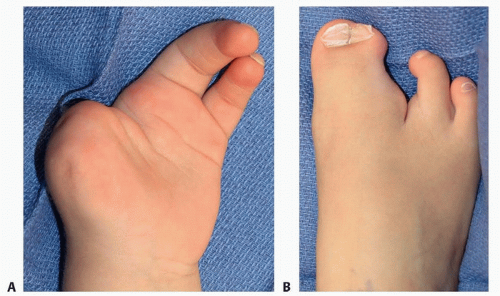
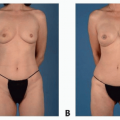
FIG 2 • This 3-year-old patient with typical cleft hand/cleft foot syndrome (the example case throughout) has two ulnar fingers but no thumb (A), as well as webbed great and second toes (B).
Variations in anatomy tend to be the rule and include deficient or missing tendons, nerves, muscles, and arteries. These variations may only become evident during the operation, and so the surgeon should be prepared with multiple contingency plans. Angiography is used more liberally in these patients.
PATIENT HISTORY AND PHYSICAL FINDINGS
A full history and physical examination should be obtained to define and document deficient anatomy, assess current functional use, ascertain associated conditions, and set goals for reconstruction.
Physical examination of the hand (FIG 2A)
The skin is inspected for suppleness, turgor, and pliability.
The soft tissue around the thumb is inspected for presence of intrinsic muscles.
Dimples in the skin may indicate underlying tendons.
Pulse examination and an Allen test are necessary to assess the blood supply to the hand and presence of palmar arch.
Physical examination of the foot (FIG 2B)
General appearance of the foot and/or toe may indicate presence of any anatomic abnormalities. In amniotic constriction bands, the toes may also be affected.
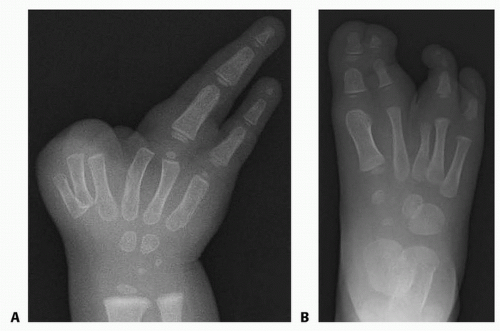
FIG 3 • Radiography of the example case shows three metacarpals on the radial side of the hand (A) and separate skeletal structures in the foot despite webbing of the great and second toes (B). Note that there are only two phalanges in the second toe. The epiphysis of the second metatarsal is not present in this early radiograph, but it is distally located in subsequent films (see TECH FIG 7A), indicating that this is indeed a phylogenetic second toe rather than a preaxial synpolydactyly.
Pulses are examined. A pencil Doppler probe can be used to ascertain the presence of an FDMA by tracing its course on the dorsum of the foot.
IMAGING
Plain radiographs of the hand and foot are required (FIG 3).
Routine angiography is debatable; nevertheless, it is the authors’ practice to obtain angiography of the hand and foot on most patients (FIG 4).
Angiography helps to create a road map and a plan for the operation. Questions such as the need for vein grafting (foot), end-to-side vs end-to-end anastomoses (hand), and residual vascularity of the foot after flap harvest can be answered preoperatively. This planning is essential in cases where a team approach with multiple surgeons is undertaken. Certainly for patients with abnormal foot anatomy (FIG 5), angiography helps with preoperative planning to ensure a viable flap.
SURGICAL MANAGEMENT
The time to perform the toe transfer should not be an arbitrary age but rather tailored to the individual child.
Although it is important to perform the transfer as early as possible to take advantage of brain plasticity and enhanced nerve regeneration, the child has to be of appropriate size to allow a technically feasible operation.
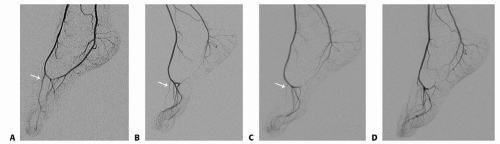
FIG 4 • Angiographic variation in arterial anatomy of the foot (FDMA indicated by white arrow). The variations outlined in FIG 1 are seen in the angiograms, with a large, dominant FDMA (A); a thinner, intramuscular FDMA (B); a diminutive FDMA (C); and no FDMA (D). The plantar system is dominant in B to D.
Specifically, the vessels tend to be too small for a predictable operation in most children under the age of 2.
The decision-making process for the parents (and the child) often requires substantial discussion. The sacrifice of part of a foot for improved function of the hand can be a difficult decision, especially when there is a small risk that the toe may not survive or that the function may not be optimal.
Thorough preparation of the parents for this process, including an honest explanation of the risks and expected outcomes, is a crucial preoperative step.
Radiographs, preoperative and postoperative photographs, molds, and movies of other patients can help with the decision-making.
Jones advocates arranging for parents to meet the families of previous patients with toe transfers.1
Multiple toe transfers are possible and can be performed reliably. Reconstruction of a thumb and finger(s) usually requires separate toes from both feet.
In contrast, multiple toes from the same foot can be used to reconstruct fingers.
Preparation of the hand recipient site with the addition of skin and soft tissue as a first-stage procedure is rarely needed in congenital cases.
However, in cases in which there is a paucity of soft tissue and skin (eg, where the base of the thumb is very short), transfer of skin via pedicled (eg, groin or lower abdomen) or free (eg, anterolateral thigh) should be considered at least 6 to 9 months before definitive toe transfer.
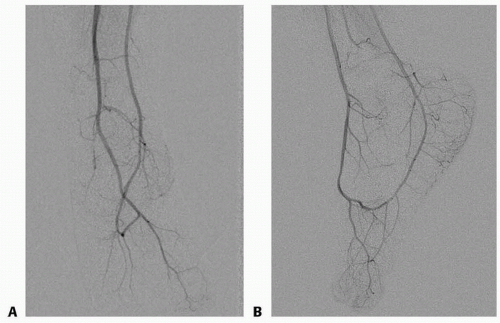
FIG 5 • Angiography of the foot of example case reveals an FDMA deep to the first dorsal interosseous supplying a single diminutive common dorsal and a single large common plantar artery. The dominant (plantar) vessel to the tibial, webbed toes lies in the web space and extends distally to the tips, sending branches along the way to both toes (A) anteroposterior view, (B) lateral view. The entire vessel was harvested with the second toe.
Skin grafting is often necessary and is much better tolerated on the hand than on the foot.
Preoperative Planning
Simultaneous dissection of the donor toe and the recipient site requires two surgical teams. This approach minimizes time of surgery and anesthesia and ensures that the critical portions of the operation take place during times when operating room staffing is optimal.Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree