Fig. 12.1 Typical sites of involvement of sclerosing disorders. Eosinophilic fasciitis and limited cutaneous systemic sclerosis both involve the extremities, but the deeper involvement of the former is evidenced by rippling of the skin. Morphea and extragenital lichen sclerosus tend to affect the trunk.
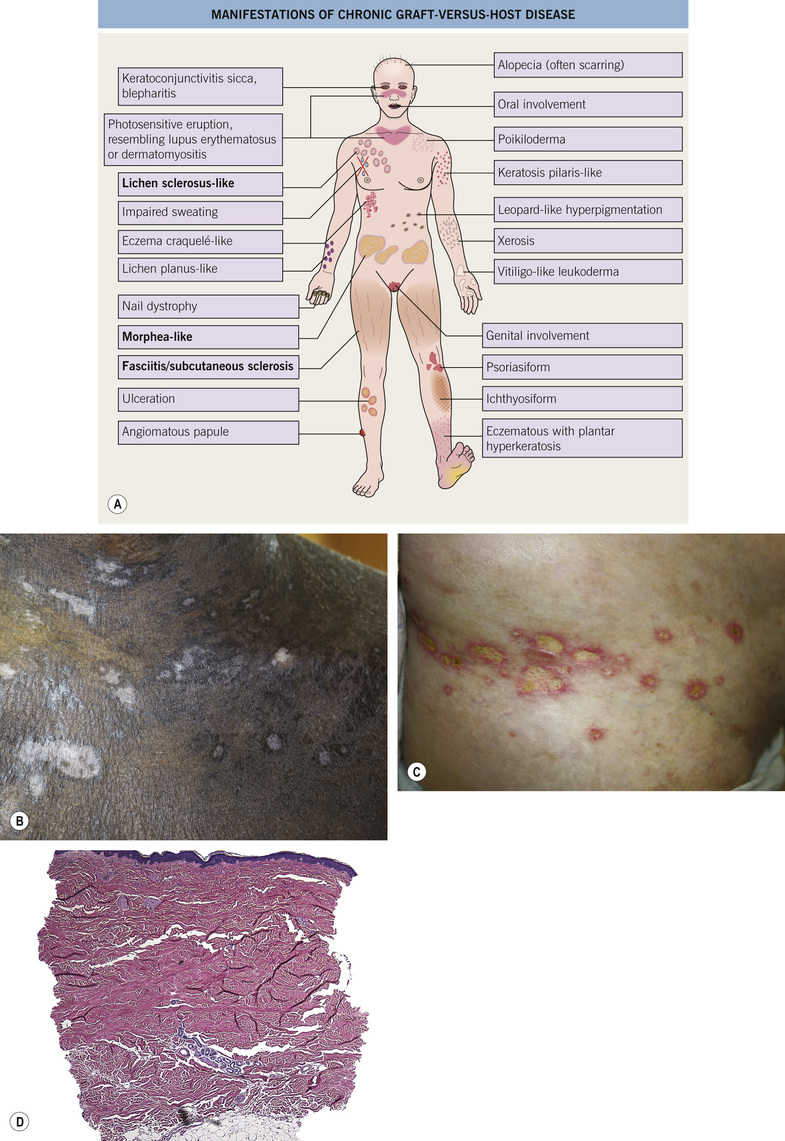
Fig. 12.2 Graft-versus-host disease. A–C Graft-versus-host disease, chronic. B Lichen sclerosus-like changes. C,D Morphea-like changes. There are superficial ulcerations. Biopsy findings are those of morphea, with sclerosis of the dermis. B,C, Courtesy, Yale Dermatology Residents’ Slide Collection. A, From Bolognia JL, Schaffer JV, Duncan KO, Ko CJ. Dermatology Essentials, 1e. Philadelphia: Saunders, 2014, with permission.
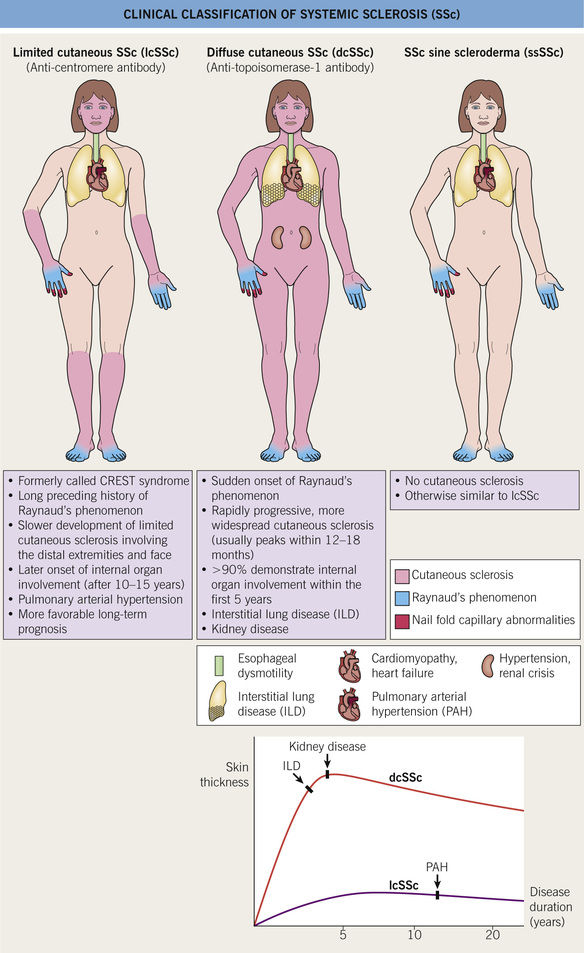
Systemic Sclerosis (Scleroderma)
Three main types of systemic sclerosis (Fig. 12.3)
Systemic Sclerosis – Clues
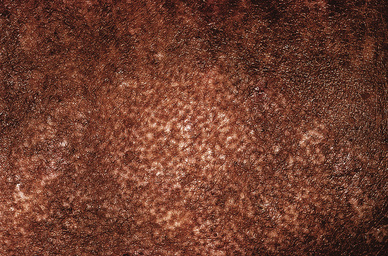
Leukoderma – retention of perifollicular pigment, producing a “salt and pepper” appearance (Fig. 12.4; see Fig. 2.26)
Acral signs – in particular, the hands can show many features suggestive of systemic sclerosis (Fig. 12.5)

Fig. 12.5 Acral signs of systemic sclerosis. A Sclerodactyly. B Scarring secondary to digital pulp infarcts. C Edematous phase of systemic sclerosis. D Calcinosis cutis. Telangiectasias. A, Courtesy, Yale Dermatology Residents’ Slide Collection; B,D, Courtesy, Kalman Watsky, MD; C, Courtesy, Jean L Bolognia, MD. B,C, From Bolognia JL, Schaffer JV, Duncan KO, Ko CJ. Dermatology Essentials, 1e. Philadelphia: Saunders, 2014, with permission.
Telangiectasias – often on the face, borders are squared off (Fig. 12.6)