Introduction
Cutaneous scars are a ubiquitous part of life; so also is the treatment of scars. Much progress has been made in therapeutic options for scars over the past few decades, as scars present notable morbidity and negative impact on quality of life. Treating scars in individuals with skin of color (SOC), particularly with energy-based devices, requires an advanced level of expertise. Individuals with SOC encompass a vast spectrum of racial and ethnic backgrounds; this can include people of African, Asian, Hispanic/Latino, Native American, and/or Pacific Islander descent. Importantly, patients with SOC have an increased incidence of postinflammatory pigment alteration (predominately hyperpigmentation; however, hypopigmentation is also possible) after dermatologic procedures due to both intrinsic and extrinsic factors. Intrinsic factors include increased epidermal melanin, larger melanosomes, and labile melanocytes and fibroblasts. Extrinsic factors include UV light and the contrast of constitutive skin color with scars that are either hyperpigmented or hypopigmented. Complications of procedural scar therapy in patients with SOC include postoperative scarring (including keloids), postinflammatory hyper- or hypopigmentation, and dyspigmentation. Because of these risks, caution with lasers, injectables, and energy-based devices is warranted to minimize epidermal injury that could then lead to postinflammatory dyspigmentation.
As medical providers, we should know how to tailor treatments and minimize risk of pigment alteration in individuals with high melanin content in their skin. It is also important to note, however, that the potential of these risks should not deter practitioners from treating scars in individuals with SOC—with caution, patients of all skin types can have great outcomes in scar therapy. This chapter reviews treatment options for three different scar types (atrophic scars, hypertrophic scars, keloids) with particular focus on how to adapt such treatments, if an adaptation is required, for patients with SOC.
Approach to Scar Management in SOC
Atrophic Scars
Atrophic scars are defined as scars that have notable dermal atrophy secondary to decreased collagen deposition after trauma or inflammation, leading to a dent or divot in the skin. Common examples of these include acne scars that can be further subcategorized as icepick (60–70%), boxcar (20–30%), and rolling (15–20%). Acne scars, which affect up to 95% of patients with acne vulgaris, have been shown to be quite distressing due to them being both aesthetically displeasing and also long-lasting. Of note, atrophic scars can also develop secondary to other inflammatory conditions including viral infections (e.g., chickenpox, smallpox), genetic conditions, surgery, or trauma.
Medical Management of Atrophic Scars in SOC
Topical therapies for atrophic scars are not often utilized in practice, as treatments such as silicone gel, silicone sheets, and topical corticosteroids only provide minor benefit. There is some evidence that topical retinoids and chemical peels may help with cell turnover and collagen stimulation in atrophic scars. In particular, trichloroacetic acid (TCA) chemical reconstruction of skin scars with 30% to 90% highly concentrated TCA can be quite effective in treating atrophic scars, especially acne scars. This treatment method provides a controlled and targeted exposure of acne scars to a high-strength chemical peel, thus stimulating collagen growth and promoting less shadowing over scar depressions. The end result is scars that are much more even in texture and less visible. In patients with SOC, caution should be taken with higher TCA concentrations due to the risk of postprocedural hyperpigmentation.
Intralesional Management of Atrophic Scars in SOC
Injectable therapies for atrophic scars include soft tissue fillers. Soft tissue fillers can be injected into atrophic scars with demonstrated effectiveness; typically, fillers with low G′ (more dense/sturdy) do best for this indication. Intralesional corticosteroids are not thought to be an ideal treatment option as they have an inherent risk of atrophy, which could of course make an atrophic scar more atrophic.
Laser and Energy-Based Management of Atrophic Scars in SOC
Laser therapy for atrophic scars includes vascular lasers, ablative fractional lasers (AFL), and nonablative fractional lasers (NAFL). Vascular lasers target hemoglobin and as such are particularly helpful for erythematous atrophic scars. Additionally, there are data showing targeted vascular destruction leads to collagen fiber heating, collagen realignment, and collagen remodeling. In SOC patients with skin phototype V or VI, one should consider longer wavelengths such as 1064 nm for treating erythema as opposed to the 532-nm potassium titanyl phosphate (KTP) or 595-nm pulsed-dye laser (PDL), both of which have the risk of destroying competing epidermal melanin.
Fractionation of ablative and nonablative devices has made laser treatments safer by decreasing bulk heating and subsequent epidermal damage. AFL include the 10,600-nm CO 2 and 2940-nm erbium:yttrium-aluminum-garnet (Er:YAG) lasers. In patients with SOC, the erbium may be better than CO 2 in mitigating risk of postinflammatory hyperpigmentation, likely secondary to decreased thermal effects of the erbium device as compared to CO 2 . Ablative devices should be used at low density in all skin types but especially darker skin tones.
NAFL encompass several different wavelengths, such as the 1927-nm thulium and the 1550-nm erbium:glass lasers. Experts tend to deem NAFL as less effective in treating atrophic scars as compared to AFL; however, they have a much safer risk profile than ablative lasers, especially in patients with SOC. NAFL may be more commonly utilized than ablative lasers for the aforementioned reasons, though generally more treatment sessions are required. Some additional modifications to consider in treating SOC patients with NAFL are keeping densities low and/or the addition of adjunctive bleaching creams or corticosteroids as well as photoprotection.
Other energy-based modalities for atrophic scars include microneedling with or without radiofrequency. Cold-microneedling is safe and efficacious in all skin types. The skin pen models are preferred to the microneedling rollers as needle channels are more reliably placed at 90 degrees to the skin. When treating with radiofrequency microneedling, the insulated needle tips are recommended in patients with SOC to reduce the risk of postinflammatory pigment alteration at the epidermal surface.
Hypertrophic Scars
Hypertrophic scars are defined as scars that are raised, sometimes red, and sometimes itchy. Importantly, these scars are confined to the border of the original trauma or surgical incision. Typically, these scars are postsurgical or traumatic in nature.
Medical Management of Hypertrophic Scars in SOC
Topical therapies for hypertrophic scars include silicone gel, silicone sheets, or hypoallergenic paper tape. Other noninvasive methods of treatment include pressure, physical therapy, and massage. For lesions that are particularly pruritic, oral antihistamines may be of benefit. Although the combination of compression and silicone has been shown to help, topical and pressure therapy alone is unlikely to be sufficient in treating hypertrophic scars in most patients.
Intralesional Management of Hypertrophic Scars in SOC
Intralesional injection with corticosteroids, 5-fluorouracil (5-FU), or a combination of the two is a commonly used modality that is quite efficacious in treating hypertrophic scars. Injections are typically performed every 4 to 6 weeks with typical doses of intralesional triamcinolone ranging from 2.5 to 20 mg/cc for scars on the face and 10 to 40 mg/cc for those on the body. The main risks of intralesional corticosteroids, especially in patients with SOC, include hypopigmentation, atrophy, and telangiectasias. Alternative injectable therapies for hypertrophic scars include 5-FU, bleomycin, and mitomycin C. In particular, triamcinolone and 5-FU are often combined—the ratio of combination often depends on the thickness of the scar, with more corticosteroid for thicker scars. Additionally, if risk of hypopigmentation from the corticosteroid is a concern, increased concentrations of 5-FU can be used. Bleomycin can be administered as multiple intralesional injections at a concentration of 1.5 IU/cc. Of note for patients with SOC, hyperpigmentation is a known risk of bleomycin injection therapy, as well as atrophy. Mitomycin C, although less commonly utilized, can be applied for 5 minutes at a concentration of 0.4 mg/cc. Overall volumes depend on surface area of the hypertrophic scar being treated.
Laser and Energy-Based Management of Hypertrophic Scars in SOC
Like with atrophic scars, lasers can be useful in treating hypertrophic scars. Vascular lasers such as PDL or KTP-crystal laser are thought to be effective in improving hypertrophic scars in two ways—both by reducing erythema and also remodeling the aberrant vasculature that contributes to the development of abnormal collagen deposition and, as a result, a hypertrophic scar. As discussed previously, caution must be taken in patients with SOC, as the hemoglobin absorption of a 585/595-nm or 532-nm laser has overlap with melanin absorption, thus increasing the risk of postprocedural dyspigmentation.
Ablative and nonablative lasers can be used in treating hypertrophic scars. Ablative lasers include the 10,600-nm CO 2 and the 2940-nm Er:YAG. AFL are considered to have the highest potential of addressing all signs and symptoms of hypertrophic scars with a single modality of therapy. In patients with SOC, the Er:YAG is considered to have a lower risk of postinflammatory hyperpigmentation as compared to the CO 2 laser, likely due to decreased thermal effects. Alternatively, NAFL offer less downtime and perhaps a decreased risk of pigmentary change. NAFL generally require more treatment sessions than AFL; NAFL are also considered to be less efficacious than AFL. Despite this, many patients and providers will still choose nonablative lasers due to their decreased downtime and lower risk profile.
The authors recommend pretreating with a compounded bleaching cream and/or topical corticosteroids for at least 1 month prior to the laser procedure. This can help reduce the risk of postinflammatory pigmentary change. General guidelines for SOC undergoing AFL or NAFL for hypertrophic scars include strict sun protection, aforementioned pretreatment adjunctive therapies, decreasing laser density +/– pulse energy, and posttreatment adjunctive topical therapies such as hydroquinone or azelaic acid. Consideration should also be given to increasing the time interval between treatments to allow any inflammation to fully subside (and therefore minimize risk of postinflammatory pigment alteration), for example, treating every 12 weeks instead of every 4 to 6 weeks.
Laser-assisted drug delivery (LADD) is becoming increasingly more common in treatment of hypertrophic scars. In LADD, AFL is followed immediately with topical application of pharmaceutical solution, typically triamcinolone or 5-FU. This method of therapy has now been established as standard practice, with numerous studies demonstrating its safety and efficacy. In a head-to-head comparison of laser-assisted delivery of triamcinolone acetonide solution versus laser-assisted delivery of 5-FU solution, 5-FU showed similar benefits of corticosteroid in treating hypertrophic scars. However, 5-FU demonstrated fewer side effects as compared to triamcinolone, which caused telangiectasias and increased scar width.
Several studies have shown that multimodal combination therapy works quite well for hypertrophic scars and in fact may be the preferred treatment method. A single treatment session could include vascular laser, AFL or NAFL, botulinum toxin A, and/or triamcinolone +/– 5-FU either injected or applied via LADD.
Surgical Management of Hypertrophic Scars in SOC
Surgery can be used for hypertrophic scars, typically as a last resort in the case of significant contraction and limitations on mobility/function. It is recommended that hypertrophic scars be given the chance to regress on their own for 1 year without surgical intervention prior to surgery being explored as a treatment option. Common surgical techniques include Z-plasty, W-plasty, or S-plasty for hypertrophic scar reconstruction. Skin grafts or local flaps may also be required. For all patients, but particularly those with highly pigmented skin, review of the risks of postinflammatory hyperpigmentation, dyschromia, and more scarring must be reviewed.
Keloids
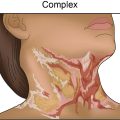
Keloids are defined as abnormal scars that extend beyond the border of the original trauma. Typically, these are erythematous, raised, and quite pruritic and/or painful. Because of this, they pose a significant amount of functional and cosmetic morbidity. For reasons still being uncovered by ongoing research, keloids are more commonly seen in individuals with skin of color, particularly those of African and Asian descent.
Most commonly, keloid scars arise from an area of previous trauma; however, spontaneous keloids can also occur, especially over the sternum. The incidence of keloids is highest in darker Fitzpatrick skin type individuals ( Box 7.1 ). Yet once keloids develop, the recurrence ratio after surgical removal is the same for all skin types. Earlobe keloids following ear piercing are the most common, but if they occur without keloids located in other anatomic areas they offer no clue as to the likelihood of the same person forming keloids elsewhere. They are usually located on the posterior lobe ( Fig. 7.1 ). When the anterior and posterior lobes are involved, the posterior lesion is usually larger ( Fig. 7.2 ). Other times, keloids wrap around the earlobe, making surgery difficult ( Fig. 7.3 ). Other common areas for keloid formation are the anterior and lateral neck ( Fig. 7.4 ), chest ( Fig. 7.5 ), abdomen ( Fig. 7.6 ), and upper back. Keloids rarely occur on the hands, feet, scalp, and axillae ( Fig. 7.7 ). Except for patients who develop keloids secondary to chemical or thermal burns and children with chickenpox, most keloids occur in the second and third decades of life. There is no known gender difference in the incidence of keloids. Keloids may be asymptomatic but are usually pruritic and may also be painful and have a burning or warm sensation.
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


