This article discusses scar contracture of the hand. It contains a brief outline of the anatomy of the hand and upper extremities and the types of injuries involved. Hand reconstruction, including examination, nonoperative treatment, surgery, excision and skin grafting, flaps, postoperative management, and complications, are covered.
The hand represents one of the most powerful sensory and functional organs of the body and separates us from other vertebrate animals through our ability to perform complex tasks. It represents a key component of almost all interactions with our environment, and serves an important role in social functioning, self-expression, productivity, and aesthetics. The hand is highly susceptible to injury. A variety of injuries may lead to contracture of the digits, wrist, and elbow. The contracture may result from simple lacerations that cross the flexion crease or web space, a postoperative infection, full-thickness skin loss, composite tissue injury, burns, crush injuries, avulsions, or amputations. Contractures across joints limit the ability to perform many of the tasks of daily living, including grasping, gripping, pinching, opening doors, getting dressed, or obtaining gainful employment.
Even small or partial functional deficits may compromise the function of the entire extremity and the quality of daily living. Scar management and revision represents a common challenge for reconstructive surgeons in the restoration of form and function.
Anatomy of the hand and upper extremities
The many specialized structures of the hand and upper extremity work in intimate synchrony to provide a harmonious interplay of precision motor biomechanics with fine tactile senses. Owing to the intricate nature these structures, there are often several components to hand stiffness and scar contracture. To appropriately treat any hand injury, one must understand each component’s involvement.
The skin of the hand is a complex organ that not only covers the underlying structures but also has specialized functional and sensory components. The glabrous palm skin can withstand shear forces and provides fine tactile sensation, whereas the dorsal skin remains mobile and permits a wide range of motion in the wrist and digits. The periarticular stabilizing structures are essential to normal joint function. These ligamentous structures, however, are prone to contracture with even limited periods of immobilization. The volar plate, collateral ligaments, tendon sheaths, and intrinsic muscles all contribute to this process. In addition, any decrease in excursion of gliding or mobile tissues, such as tendons, can result in significant compromise. Splinting, edema control, and early motion guided by hand therapy are the key to the prevention and treatment of contractures of the hand and upper extremity.
At the core of hand function is the bony support and articular surfaces. Any fractures or articular injury can lead to tendon imbalance, alteration of joint biomechanics, and mechanical obstruction. Proper treatment and healing is necessary to allow early range of motion and hand therapy. Both are keys in preventing and treating soft tissue contraction and subsequent contracture.
Joints are the areas of greatest motion in the hand. The metacarpal phalangeal (MCP) joint is a condyloid joint with three planes of motion, including flexion or extension, adduction or abduction, and rotation. The collateral ligaments arise dorsal to the axis of rotation, and with the volar flare of the metacarpal head, provide a cam effect. Thus, there is the least amount of joint space and the most stretch on the collateral ligaments during flexion and the greatest amount in extension. Swelling increases the volume of fluid within the joint and forces the MCP joint into extension in which the collateral ligaments contract to their shorter position and make flexion difficult. Following acute trauma, therefore, the MCP joint should be splinted in flexion to prevent collateral ligament contracture.
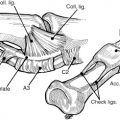
The proximal interphalangeal (PIP) joint is a hinge joint with 0° to 100° of flexion. Here, the collateral ligament originates at the center of rotation, so there is no Cam effect and tension is equal throughout the arc of motion ( Fig. 1 ). The accessory collateral ligament inserts onto the volar plate, so there is the least amount of joint space and the most stretch on the ligaments during extension. The volar plate is also at greatest stretch during extension of the PIP joint. The PIP joint should be splinted in extension following acute trauma or in conditions of acute or chronic swelling.

Initial examination for hand and upper extremity injury
The history and cause of the injury are important in assessing the potential structural involvement and previous interventions. This will provide the framework in which to begin treatment. Also important is the patient’s medical and social history, which may reveal potential factors contributing to wound healing problems and increased scar propensity Box 1 .
Factors and Conditions in Wound Healing and Scar Formation
Wound
Contamination
Infection
Delayed closure
Wound tension
Wound location (trunk, chest)
Sun exposure and UV damage
Immobilization
Swelling
Host
Skin type
Keloid history
Radiation history
Malnutrition
Vascular disease
Smoking
Diabetes
Connective tissue disorders (Dupuytren disease)
Arthritis
Autoimmune disorders
Patient compliance/therapy
The physical examination of the scarred hand and upper extremity involves a systematic evaluation. The neurovascular status should be examined throughout the able range of motion. Structural integrity is also assessed, first clinically by deformity, palpation, tenderness, and then radiographically though radiograph, CT scanning, and angiography, as necessary. Most important in the secondary scar release is a functional assessment, including a detailed motor and sensory examination. First, passive and active ranges of motion are evaluated. A greater composite range of motion is required on the ulnar aspect of the hand for power grip, while less can be tolerated in the thumb and index and long fingers where key pinch is required. Initially, an assessment of the skin should be performed and any areas of tightness or limited mobility documented. Next, testing of intrinsic tightness with the Bunnell-Francescetti intrinsic tightness test will elucidate the cause of any additional limitations in range of motion, such as intrinsic or extrinsic musculotendinous tightness. This test assesses the MCP motion’s effect on PIP motion. If PIP motion is improved with MCP flexion, the test is positive for intrinsic tightness. If PIP motion is improved with extension, the limitation can be attributed to the extrinsic extensors.
Initial examination for hand and upper extremity injury
The history and cause of the injury are important in assessing the potential structural involvement and previous interventions. This will provide the framework in which to begin treatment. Also important is the patient’s medical and social history, which may reveal potential factors contributing to wound healing problems and increased scar propensity Box 1 .
Factors and Conditions in Wound Healing and Scar Formation
Wound
Contamination
Infection
Delayed closure
Wound tension
Wound location (trunk, chest)
Sun exposure and UV damage
Immobilization
Swelling
Host
Skin type
Keloid history
Radiation history
Malnutrition
Vascular disease
Smoking
Diabetes
Connective tissue disorders (Dupuytren disease)
Arthritis
Autoimmune disorders
Patient compliance/therapy
The physical examination of the scarred hand and upper extremity involves a systematic evaluation. The neurovascular status should be examined throughout the able range of motion. Structural integrity is also assessed, first clinically by deformity, palpation, tenderness, and then radiographically though radiograph, CT scanning, and angiography, as necessary. Most important in the secondary scar release is a functional assessment, including a detailed motor and sensory examination. First, passive and active ranges of motion are evaluated. A greater composite range of motion is required on the ulnar aspect of the hand for power grip, while less can be tolerated in the thumb and index and long fingers where key pinch is required. Initially, an assessment of the skin should be performed and any areas of tightness or limited mobility documented. Next, testing of intrinsic tightness with the Bunnell-Francescetti intrinsic tightness test will elucidate the cause of any additional limitations in range of motion, such as intrinsic or extrinsic musculotendinous tightness. This test assesses the MCP motion’s effect on PIP motion. If PIP motion is improved with MCP flexion, the test is positive for intrinsic tightness. If PIP motion is improved with extension, the limitation can be attributed to the extrinsic extensors.
Treatment of scar contracture
The initial treatment of any soft tissue scar contracture is optimization through nonoperative management and aggressive physical therapy. The nonoperative interventions include scar massage, compression therapy, silicon sheeting, static or progressive casting, steroid injection, assisted range of motion, and a variety of orthosis techniques, such as serial casting. Surgical intervention is discussed when no additional improvement is expected with the conservative methods. Typically soft tissue equilibrium has been achieved for at least 6 months.
Surgical intervention
The goal of procedures designed to release contractures of soft tissue are to improve the motion, sensibility, durability and overall function of the hand. The contracture release procedures should be timed appropriately with consideration given to other potential interventions that may require splinting or immobilization that may interfere with the release. Attempting to address too much in one stage carries a significantly higher risk of postoperative pain, edema, and poor outcomes. The most common releases permit extension of the digits, wrist, elbow, or axilla, widening of the first web space, resurfacing of unstable scars, or restoring a sensate pad to finger tips.
Excision and skin grafting
Scar incision or excision may result in a significant soft tissue defect that extends beyond the capacity of local flaps. Skin grafts are often used to cover the wound bed following scar excision. Full-thickness grafts are usually used on the volar aspect of the hand to limit the recurrence of contractures.
Transposition flaps
Many minor or moderate contractures can be corrected with local skin flaps, avoiding the need for skin grafts or more extensive procedures. Transposition flaps are commonly used to correct these contractures. Z-plasties are normally oriented at 60° for each limb, which provides a 75% increase in length of the central limb; however, many angle modifications exist ( Fig. 2 ). The larger the angle at the apex of the Z-plasty, the more gain in length is achieved in the contracture release. The increase in this angle, however, puts greater the tension on closure and greater is laxity needed in the perpendicular plane. It is often better to use multiple Z-plasties in sequence ( Figs. 3–5 ). When the two limbs are unequal or nonparallel, it is more properly called a transposition flap.
Square, double, 4-flap, 5-flap, 6-flap ( Fig. 6 ), and jumping man ( Fig. 7 ) Z-plasties are all modifications of this procedure and are demonstrated below with additional information on length gain Table 1 .
| Theoretical Increase in Central Limb for Various Z-Plasties | ||
|---|---|---|
| Type of Z-Plasty | Percentage Increase in Central Limb (%) | New Length of Central Limb a (cm) |
| Simple Z-plasty with 45° | 50 | 1.5 |
| Simple Z-plasty with 60° | 75 | 1.75 |
| Simple Z-plasty with 75° | 100 | 2 |
| 4-flap Z-plasty with 45° | 100 | 2 |
| 4-flap Z-plasty with 60° | 150 | 2.5 |
| 6-flap Z-plasty with 45° | 150 | 2.5 |
| Double-opposing Z-plasty | 75 | 1.75 |
| 2 Z-plasties in series | 75 | 1.75 |
| 5-flap Z-plasty | 125 | 2.25 |
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


