Scalping Forehead Flap
J. G. McCARTHY
EDITORIAL COMMENT
This is one of the best techniques for total nasal reconstruction. The editors caution the surgeon to have all preliminary reconstructions completed, so that the only defect left to reconstruct is the nose itself. The skin-grafted defect left in the forehead may be eliminated with tissue expansion of the forehead at a later time.
The scalping forehead flap, described by Converse in 1942 (1, 2), represents the logical extension of the classical (Indian) forehead flap in nasal reconstruction. This flap satisfies requirements for length and, in addition, delivers a large area of forehead skin of satisfactory color and texture match for nasal reconstruction.
INDICATIONS
The scalping flap is a reliable technique for reconstructing large nasal defects. The flap skin is supple enough to be folded to recreate the lobular portion of the nose. The flap design provides the desired length for reconstruction of the columella, and the reconstructed nose thus has adequate size and projection.
The main disadvantage of this flap is the residual forehead donor defect. This is easily camouflaged in females, however, by an appropriate hairstyle. The skin graft can be reduced in size by serial excision or by replacement with local skin transferred either as a Schimmelbusch (3) or Juri (4) flap.
ANATOMY
The forehead scalping flap includes the forehead skin, the scalp and galea, and a major portion of the vasculature of the forehead and anterior portion of the scalp.
The frontalis muscle, the galea, and their overlying integument are vascularized by an extensive anastomotic network from the supraorbital, supratrochlear, and superficial temporal vessels (Fig. 56.1). All these vessels, with the exception of the superficial temporal system on the ipsilateral side of the flap, ensure a rich blood supply to the flap.
The venous drainage is remarkably efficient. The supraorbital veins, which run superficial to the frontalis muscle, communicate with the anterior branch of the superficial temporal vein. The superficial temporal vein drains the upper portion of the flap into the posterior facial vein. The supraorbital vein joins with the supratrochlear vein at the medial angle of the orbit to form the angular vein.
The frontalis muscle, which is not included in the flap (see Fig. 56.5), is a thin quadrilateral muscle intimately adherent to the superficial fascia. Its vertically oriented fibers are pale in color. The medial margins, joined above the root of the nose, gradually diverge from each other, leaving a muscular gap in the central portion of the forehead.
FLAP DESIGN AND DIMENSIONS
In planning the procedure, the surgeon must first define the nature and extent of the nasal defect to be resurfaced by the
flap. A wool or flannel cloth pattern of the defect is made and transferred to the lateral aspect of the selected side of the forehead. In the male with a receding hairline, the donor area on the forehead should be positioned as far laterally as possible to camouflage the donor site when the patient’s full face is observed.
flap. A wool or flannel cloth pattern of the defect is made and transferred to the lateral aspect of the selected side of the forehead. In the male with a receding hairline, the donor area on the forehead should be positioned as far laterally as possible to camouflage the donor site when the patient’s full face is observed.
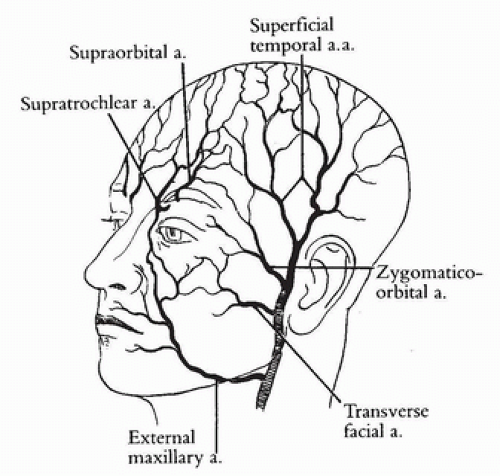 FIGURE 56.1 Blood supply of the forehead. Most forehead flaps are axial-pattern flaps based on the superficial temporal, supraorbital, and supratrochlear vessels. (From Converse, ref. 8, with permission.) |
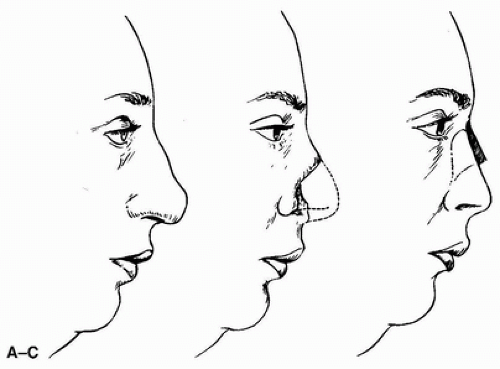 FIGURE 56.2 Reduction of the residual nasal stump prior to subtotal nasal reconstruction. If the nose was large prior to amputation (A), it is advantageous to reduce the projection of the residual stump (B) to facilitate nasal reconstruction (C). (From Converse, ref. 8, with permission.) |
It must be emphasized that if the residual stump is that of a large nose, its size should be reduced, because it is technically simpler to build a smaller nose than a large one (Fig. 56.2). When the lobular portion of the nose, including the columella and alar rims, is to be replaced, the distal end of the flap is folded on itself (see Fig. 56.10). Consequently, the working portion of the flap should be of sufficient size to allow such a degree of flap fashioning.
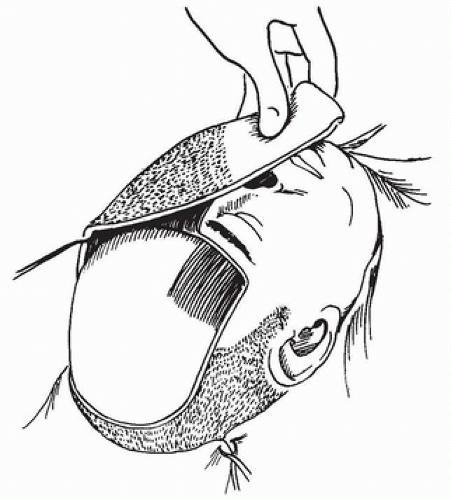 FIGURE 56.3 To reconstruct the tip of the nose, columella, and alae, the flap must be sufficiently long to reach the lower lip prior to insetting. (From Converse and McCarthy, ref. 2, with permission.) |
While the shape of the pattern had been roughly triangular in the past (narrower above than the wider distal portion), a rectangular design has been employed in recent years.
When reconstructing the lobular portion of the nose, it is a good rule to be able to advance the flap to the lower lip without tension in order to have a columella of adequate length and a nasal tip of sufficient projection (Fig. 56.3).
While the lining flaps maybe multiple in origin, the covering cutaneous flap should ideally restore the entire aesthetic unit. In resurfacing the nose, the surgeon should strive to design the flap so that it extends from the most distal portion of the nasal tip and the borders of the alae to the root of the nose. This is especially important along the dorsum of the nose, where a transverse junction line (scar) between the flap and the dorsal skin is obvious. The junction scars between a central flap and the adjacent lateral aspect of the nose (or cheek) are less conspicuous.
Related posts:
 Cheek Rotation Skin (Mustardé) Flap to The Lower Eyelid
Cheek Rotation Skin (Mustardé) Flap to The Lower Eyelid
 Nasalis Musculocutaneous Sliding Flaps for Nasal Tip Reconstruction
Nasalis Musculocutaneous Sliding Flaps for Nasal Tip Reconstruction
 Oral Mucosal Flaps for Septal Reconstruction
Oral Mucosal Flaps for Septal Reconstruction
 Postauricular and Retroauricular Scalping Flap (The Paras Flap)
Postauricular and Retroauricular Scalping Flap (The Paras Flap)
 Scapular and Parascapular Flaps
Scapular and Parascapular Flaps
 Platysma Musculocutaneous Flap to The Lower Lip
Platysma Musculocutaneous Flap to The Lower Lip
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


