This article describes the background and importance of scalp reconstruction. The relevant anatomy and neurovasculature will be discussed. Finally, the entire reconstructive ladder will be examined in its relation to scalp reconstruction and how to optimally reconstruct scalp defects.
Key points
- •
The scalp is a unique and essential region of the head and neck that provides the first barrier to the cranium and the brain.
- •
Reconstruction of the scalp can be challenging due to the convexity and relative inelasticity.
- •
A variety of methods can be used to reconstruct scalp defects and the best technique should be chosen on a case-to-case basis as this will depend on both defect and patient characteristics.
Introduction
The scalp is a complex anatomic structure that is essential for many physiologic functions in the body. The scalp serves not only as the first barrier to the calvarium and the brain beneath, but it is also one of the most exposed areas of our bodies, which has both functional and cosmetic implications. Because of this, adequate reconstruction of defects is a priority.
The scalp functions as an initial barrier to protect the skull from external elements and trauma. Defects including calvarium and/or dura introduce the risk for cerebrospinal fluid leak, meningitis, or brain abscess. Larger calvarial defects may also lead to the “syndrome of the trephined,” an array of neurologic symptoms caused by either atmospheric pressure compressing the brain or changes in cerebrospinal fluid circulation. , Reconstruction of the scalp is necessary to prevent these complications that develop when the scalp no longer provides its function.
While restoring the scalp’s function as a barrier is a primary goal of reconstruction, restoring cosmesis becomes an important secondary goal. This is due to the exposed nature of the scalp making abnormalities easily noticeable. Cosmetic outcomes include scalp contour and color match, both of which can affect patient psychology and quality of life. The scalp also presents unique cosmetic considerations because it contains hair-bearing and non-hair-bearing skin. As such, preventing alopecia should also be a consideration during reconstruction.
Scalp defects can be created in numerous ways but are most commonly from tumor extirpation (malignant and benign) or trauma. If malignancy is present, negative margins should be achieved prior to reconstruction. Reconstruction of the scalp can be challenging due to the thickness of the scalp tissue and inelasticity. There are many options available for reconstruction of these defects, all with their own advantages and disadvantages. These techniques range from primary closure to secondary intention to free tissue transfer.
This study describes the anatomy and neurovasculature of the scalp necessary for the reconstructive surgeon. Additionally, this study goes into detail regarding the management of scalp defects, including each rung of the reconstructive ladder and when each option is indicated.
Anatomy
In order to attain the best possible result, the reconstructive surgeon should have a thorough understanding of scalp anatomy. The scalp consists of 5 layers that are (from superficial to deep) the skin, subcutaneous tissue, galea aponeurosis, loose connective tissue, and pericranium. The skin and subcutaneous tissue are densely adherent to the galea, which contributes to the inelasticity of the scalp. This inelasticity can make primary closure more difficult. The vasculature, innervation, and hair follicles of the scalp lie in the subcutaneous layer. The galea is a layer of thick connective tissue that is continuous with the frontalis anteriorly, temporoparietal fascia laterally, and the occipitalis posteriorly. 76 The loose connective tissue layer is an avascular plane between the galea and underlying pericranium. Because of this, the loose connective tissue layer is the most ideal layer for dissection in order to elevate flaps and mobilize the scalp. Lastly, the pericranium provides blood supply to the calvarium and also provides a vascularized layer that can facilitate healing via secondary intention or a bed for a skin graft. The calvarium consists of both an inner and outer table with a diploic space in-between.
The vertex of the scalp is the least mobile area of the scalp with the lateral areas being the most mobile. This means that the parietal scalp may be most amenable to primary closure, while the vertex may require other techniques to achieve closure.
Many patients, especially those with cutaneous malignancies, present at later stages in life. The mean age at presentation for squamous cell carcinoma of the skin is 70 years old and is most commonly due to cumulative sun exposure. Because of this, many patients undergoing scalp reconstruction are in older age groups, and thus, the condition of the aging scalp must be considered.
As scalp skin ages, the epidermis becomes thinner and the skin becomes less elastic, especially in female individuals. Intrinsic factors such as telomere shortening, decreased collagen and elastin production, and cumulative oxidative stress contribute to these skin changes. Extrinsically, ultraviolet radiation is the primary factor, while tobacco smoke, menopause, or inflammatory disorders may also affect the scalp skin.
For the reconstructive surgeon, this may exaggerate the steps needed to reconstruct a defect. For primary closure, more undermining may be required. For rotational flaps, larger flaps may need to be designed. Many times, the lack of elasticity and thinness of the skin may predispose this group of patients for free tissue transfer that may have been able to be closed with less invasive methods of reconstruction.
Neurovasculature
The scalp is supplied by 5 paired blood vessels arising from both the internal and external carotid systems that form an anastomotic plexus centrally. These vessels include the supratrochlear and supraorbital arteries anteriorly, the superficial temporal and postauricular arteries laterally, and the occipital arteries posteriorly. The venous drainage of the scalp corresponds to these arteries and drains both into the external and internal jugular veins. Innervation of the scalp is provided by branches of both the trigeminal nerve and the cervical plexus. Knowledge of the neurovascular elements of the scalp is essential to proper flap design for both local and regional flaps.
Secondary intention
The simplest form of scalp reconstruction is by secondary intention with local wound care. Secondary intention is when the wound is left to heal naturally via granulation. This may take the longest time in terms of healing compared to the other methods of reconstruction; however, relatively good results can be achieved, especially in non-hair-bearing skin. This technique is primarily used in relatively superficial wounds. As mentioned previously, elderly patients have thinner and less elastic skin that may preclude primary closure or local flap reconstruction, making secondary intention a possible option in this population. Because of this thin skin in the elderly population, these patients are also more susceptible to scalp trauma that may present as deeper than expected wounds or with exposed bone.
Secondary intention works best when pericranium is present to provide a bed for granulation tissue, but if it is not present, the outer table can be drilled to the diploic space to provide a vascular bed for granulation tissue. Temporoparietal fascial flaps or pericranial flaps can be created to replace the pericranium if needed. Additionally, a skin substitute is a collagen matrix that can be used to stimulate wound and create a more robust bed of granulation tissue for secondary intention. Many of these wounds will go on to require a split-thickness skin graft at a later time.
The limitations of this technique are the time required for healing and the need for consistent wound care by the patient or caregiver. This option is not ideal for patients who are not able to care for themselves or may not be able to perform the regular wound care. Prior radiation may also be a relative contraindication as the vascularity has been significantly reduced making secondary intention either extremely slow or not possible. Additionally, the final wound may be depressed relative to nearby tissue, alopecic if done in an area of hair-bearing scalp, and can be hypopigmented. In general, wounds heal very well via secondary intention despite a long healing time, rarely are complicated by infection or tissue breakdown, and usually result in high patient satisfaction with their outcome.
Primary closure
The next option for reconstruction is primary closure and can lead to the best cosmetic result if done properly. Primary closure is the direct apposition of wound edges. This is typically performed by placing subcutaneous sutures, followed by a superficial skin closure, whether suture or staples. Staples are typically reserved for hair-bearing scalp but removal is typically tolerated less well. The author’s preference is for absorbable suture to prevent any need for removal. Primary closure minimizes alopecia and is best done in patients with higher skin mobility.
For primary closure to be achieved, defects are typically made elliptical in shape and a significant amount of subgaleal undermining is required. One study has shown that undermining can reduce tension on the closure by 83.3% and 92.2% for 5 cm and 15 cm of undermining, respectively. In elderly patients, the amount of undermining needed is best performed in areas of higher skin mobility and the relation of the nearby hairline must be taken into account. Significant tension in closure should be avoided as high tension closures can lead to wound dehiscence and scar widening. ,
Galeotomies or rapid intraoperative tissue expansion can be performed to reduce wound tension and increase advancement of the skin. , An example is shown in Fig. 1 . Rapid intraoperative tissue expansion does not produce more collagen but instead relies on the principle of mechanical creep. This process deforms the 3 dimensional structure of collagen fibrils, which allows for an increase in length. Rapid intraoperative tissue expansion is typically performed by placing a Foley catheter under the skin adjacent to the defect and inflating the balloon for 5 minutes. Doing so allows for an increased length of the opposing wound edges and reduced wound tension. On the other hand, galeotomies are performed by making incisions on the undersurface of undermined skin flaps parallel to the defect. Doing so reduces closing tension with each galeotomy; thus, more galeotomies may produce increased length and lower tension of the final closed wound.

Skin grafting
Split-thickness or full-thickness skin grafts may also be used for scalp reconstruction. These techniques are both reliable and relatively simple. Split-thickness skin grafts are grafts that include the epidermis and superficial dermis, while full-thickness skin grafts include the entire dermis and epidermis.
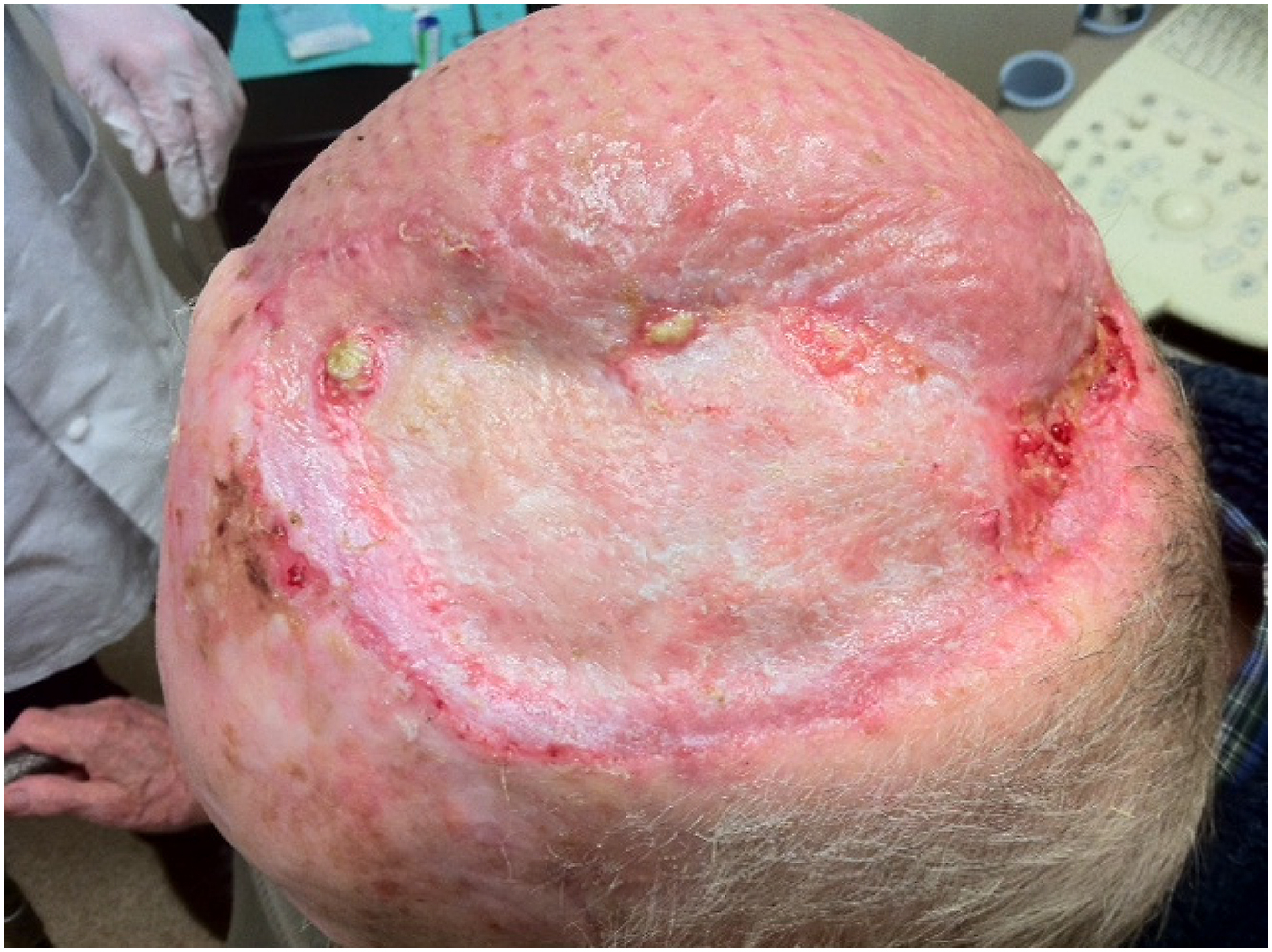
Split-thickness skin grafts may be harvested from the thigh, abdomen, or buttocks. These grafts may be meshed to allow coverage of a larger surface area with smaller grafts. Full-thickness skin grafts may be harvested from the postauricular area, preauricular area, or supraclavicular area. Subcutaneous fat must be removed from full-thickness grafts as this fat may inhibit revascularization. Skin grafting may be especially useful in patients who are not appropriate candidates for more extensive surgery or patients who have a high risk of recurrence after resection of a malignant tumor. A split-thickness graft may be preferred for larger defects in which grafting is to be used as it is easier to harvest larger areas of this type of graft compared to full-thickness. An example of a healed split-thickness skin graft is shown in Fig. 2 . Current literature shows no differences in skin graft take or complications when comparing split-thickness to full-thickness grafts for scalp reconstruction.
The key to using a skin graft is placement onto well-vascularized tissue, whether that is pericranium, drilled calvarium, or a pericranial/temporoparietal fascial flap. Thus, if pericranium is absent, the calvarium may be drilled (as described earlier) to provide a vascularized wound bed. A skin graft cannot be used in a radiated field or if radiation is planned postoperatively. Skin grafts have a high risk of breaking down if subjected to radiation after placement. Esthetically, skin graft outcomes are similar to secondary intention and are characterized by hypopigmentation, depression, and alopecia.
Additionally, skin substitutes may be used in nonhealing scalp wounds, radiated tissue beds, or to generate granulation tissue for skin graft take. Skin substitutes typically contain a collagen matrix that is placed and allowed to granulate over the course of several weeks. At this point, a skin graft may be placed in a patient who may otherwise not have been able to receive one.
Local flaps
The use of local tissue from the surrounding skin of a scalp defect is an excellent option for small-to-medium-sized defects. These can be designed as advancement, pivotal, or interpolated flaps. Incisions for these flaps should be designed to maximize the vascularity of the flap and should always be made with the anterior hairline in mind. Local flaps are raised in the subgaleal plane. As with primary closure, raising local flaps on the scalp typically requires more extensive undermining and longer incisions than other areas of the head and neck in order to achieve the necessary mobility of the flap. The scalp and forehead should be treated as separate esthetic subunits and defects that involve both should be repaired with separate flaps for each subunit.
Due to the inelasticity of the skin, advancement flaps are less useful on the scalp than other regions of the head and neck. Typically, pivotal flaps have more use due to the spherical shape of the cranium. Pivotal flaps can be rotational, interpolated, or transpositional. An example of a rotational flap is shown in Fig. 3 . Curvilinear incisions are made and relatively small defects often require much longer incisions, ranging from 4 to 6 times the diameter of the defect. Because of this, multiple flaps may be needed to cover larger defects. A standing deformity will typically form at the fixed point of rotation. This should be left in place and excised later as excision may compromise blood supply by narrowing the base of the flap. , Larger local flaps may lead to the development of a secondary defect of the donor site/base of the flap. Because this secondary defect is usually in a more inconspicuous location, it may be left to heal via secondary intention, skin graft, or closed with additional local tissue advancement. Incisions may be hidden in skin creases or along hairlines. Additionally, incisions should be made parallel to the direction of hair follicle growth to reduce the risk of alopecia. Local flaps appear to be time efficient, achieve adequate coverage with hair-bearing skin, and have low complication rates.









