87 Scalp Extension and Triple-Flap Techniques to Treat Extensive Baldness
Summary
Keywords: scalp extender scalp extension scalp reduction slot deformity Frechet’s triple-flap technique
Key Points
•Scalp extension and triple-flap technique provide a reliable option for the management of Norwood stage VI and VII baldness.
•The novice should not attempt transposition flaps until a minimum of 10 to 20 scalp extension procedures have been performed.
•A strict respect for flap dimensions and the avoidance of excessive tension are extremely important to minimize problems with the triple-flap procedure.
87.1 Introduction
Extensive baldness, Norwood stage VI and VII, affects a great number of patients. The use of grafts alone to treat these patients is inadequate for a full and satisfactory hair coverage. An average of 80 hairs/cm2 are necessary to cover significantly a 300 cm2 bald area. This represents a total of 24,000 hairs. Such number of hairs is not achievable with grafts alone. For these patients, the author uses, for the past 30 years with great satisfaction and safety, the scalp extension and triple-flap techniques to treat the two posterior thirds of the bald area and grafts for the frontal zone. The whole treatment requires four procedures over a 4-month time period. It allows patients to lead a normal everyday life during the whole process of treatment. To accomplish this task, an extender device plays a major role.
87.2 Description of the Scalp Extender and Its Mechanism of Action
The scalp extender1 is a thin rectangular sheet of silicone elastomer with a row of hooks on the two lateral ends (Fig. 87.1). This sheet has elastic properties that enable it to stretch by 100 to 200% with a natural tendency to return to its original size.
Fig. 87.1 Frechet’s extender.
The extender is stretched and affixed to the underside of the galea from one side of the parietal hair-bearing scalp to the other, and remains in position until it returns eventually to its original size. Consequently, this device stretches the laterally based hair-bearing tissue, resulting in a contraction zone within the bald tissue surface located between the opposing rows of hooks. The property of contractility generated within the bioelastic material stimulates biological “creep” in the adjacent, hair-bearing soft tissue.
The donor zone for the future harvest in not affected by these procedures as the hair density of the occipital scalp is unchanged after scalp extension. The scalp extension process stretches only the lateral sides of the scalp and not the occipital area where grafts will be later harvested.
87.3 Description of a Typical Operation
87.3.1 Initial Phase: Insertion of the Extender
The procedure is performed under local anesthesia. An elliptical midline scalp reduction is performed, removing an alopecic zone typically measuring 3- to 4-cm wide by 15 to 20 cm or more in length. The scalp is then undermined beneath the galea. Before closing the scalp, the row of hooks on one end of the extender is engaged to the underside of the galea at one edge of the incised scalp. The bioelastic device is stretched with a needle holder and the opposite row of hooks are engaged into the contralateral galeal undersurface. For example, if a 4-cm-wide ellipse of alopecic tissue is excised from a bald area measuring 15-cm wide, an 11-cm-wide zone of bald scalp will remain. A 4-cm-length extender will be stretched to a total of 11 to 12 cm following its hook insertion into the galea at both edges of the midline reduction. The elastic recoil forces of the extender lead to its gradual retraction, which culminates in stretching the hair-bearing scalp lateral to the hook-insertion points.
87.3.2 Extender Removal Phase
When the patient returns for surgery, usually 4 to 6 weeks later, various phenomena can be noted:
•There is no unsightly volumetric modification of the head, such as that seen with expanders.
•A decrease in the width of the central baldness often measuring 8 to 11 cm has been achieved. This “shrink-back”-induced alopecic reduction is a unique phenomenon of the extender.
•The scar is finer than that seen with the conventional method of alopecia reduction. The absence of any tension on the line of closure throughout the “shrink-back” process is largely responsible for this.
The second operation is performed, for the most part, in a similar fashion as the first part. A second scalp reduction is performed, and a 3-cm-length extender is inserted for this second procedure. Then the scalp is closed, typically leaving about 5 cm in width of remaining alopecia from an initial pretreatment width of 15 cm.
The residual alopecic slot typically measures about 2.5-cm wide 4 to 6 weeks following placement of the second extender. Now is the time for the third procedure where the extender will be removed and the slot eliminated using three hair-bearing transposition flaps to position the hairs in a natural direction. A third extension can be performed immediately after the second for those with a tight scalp and a slot wider than 2.5 cm.
87.4 Scalp Extension for Beginners
The key to successful scalp extension for the novice is to avoid complications. Initially, it is wise to avoid treating baldness greater than 15 cm in width. Complications, if ever, are most common with the initial 10 to 20 triple-flap procedures. Prior to attempting the triple-flap procedure, it is recommended that the surgeon first become fully comfortable with scalp extension surgery. No transposition flaps should be attempted until a minimum of 10 to 20 scalp extensions have been completed. These first patients are best managed by first completing two sequential midline alopecia reductions using scalp extenders. When removing the second extender 8 to 12 weeks after the beginning of treatment, a final elliptical reduction is designed, which should terminate 3.5 cm anterior to the posterior boundary of the previous reduction (Fig. 87.2a, b). This method avoids creating a slot, but instead leaves a small pear-shape bald spot in the occipital area that can be easily transplanted with grafts 3 or more weeks later.2 Using scalp extension alone, the top and back baldness will have yet shrunk from 200 to about 30cm2. Some doctors may continue with this approach alone without the triple-flap procedure and never have problems to fear.
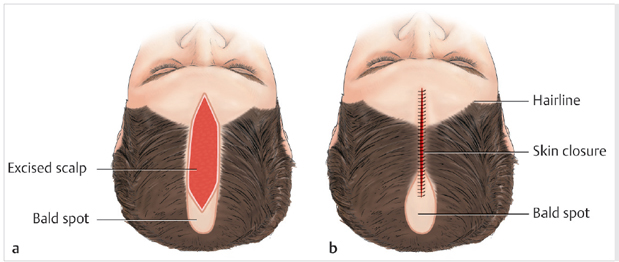
Fig. 87.2 (a) For patients who will not undergo the triple-flap procedure, the final scalp reduction ellipse should terminate 3.5 cm anterior to the posterior boundary of the previous reduction. (b) A small pear-shape alopecic area will remain at the posterior end of the reduction site, which can be managed with later grafting.
Related posts:
 The Patient with Minimal Hair Loss: Planning and Decision-Making
The Patient with Minimal Hair Loss: Planning and Decision-Making
 Hair Anatomy and Histology for the Hair Transplant Surgeon
Hair Anatomy and Histology for the Hair Transplant Surgeon
 Plugged in: How to Ensure That Your Practice Thrives (and Survives) in Today’s DigitalWorld
Plugged in: How to Ensure That Your Practice Thrives (and Survives) in Today’s DigitalWorld
 Recreating the Vertex
Recreating the Vertex
 Transplanting into Areas of Cicatricial Alopecia
Transplanting into Areas of Cicatricial Alopecia
 Special Considerations for Postoperative Care in Follicular Unit Excision
Special Considerations for Postoperative Care in Follicular Unit Excision
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


