Fig. 4.1
Dermoscopy image of lentigo maligna melanoma on the cheek displaying an annular-granular pattern composed of gray and brown dots asymmetrically distributed around follicular openings
UVR damaged skin of the torso and extremities differs from facial skin in that it usually has some preserved rete ridges and significantly fewer adnexal openings [10]. Thus, LM/LMM on non-facial sun damaged skin often reveals focal islands of network without an annular granular pattern.
One dermoscopic feature commonly seen in LMM, irrespective of anatomical location, is the presence of angulated lines. These angulated lines can coalesce to create zigzag lines and polygons. On facial skin the most common polygons formed are rhomboidal structures (Fig. 4.2). In contrast, on non-facial sun damaged skin the polygons tend to be larger than those on facial skin and can take on polygonal shapes other than rhomboids (Fig. 4.3) [1, 10].
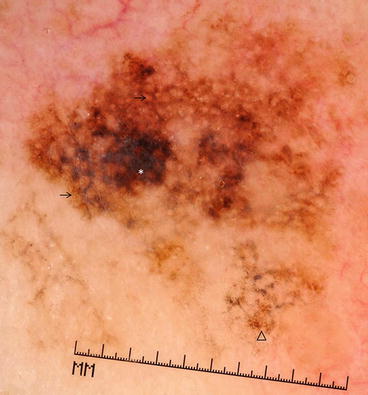
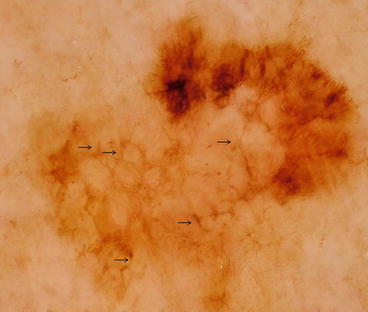
Fig. 4.2
Dermoscopy image of lentigo maligna melanoma on the cheek. Note angulated lines (arrows) leading to formation of rhomboidal structures, regression/granularity (triangle), and central blotch (white asterisk) with obliterated follicular openings
Fig. 4.3
Dermoscopy image of lentigo maligna melanoma on the shoulder. Note numerous angulated lines (arrows) that form polygonal structures including rhomboids
Dermoscopic Features of LM/LMM
The classic LM/LMM dermoscopic specific structures include:
Asymmetric distribution of pigment, often with grayish hues, surrounding follicular openings (Fig. 4.3). This corresponds on histopathology to the presence of atypical melanocytes in the epidermis that are surrounding and/or descending into the hair follicles [8]. In addition, concentric pigmented circles surrounding follicular openings may be present. This feature is called the isobar structure or the circle-within-a-circle structure (Figs. 4.4, 4.5, and 4.6) [1].
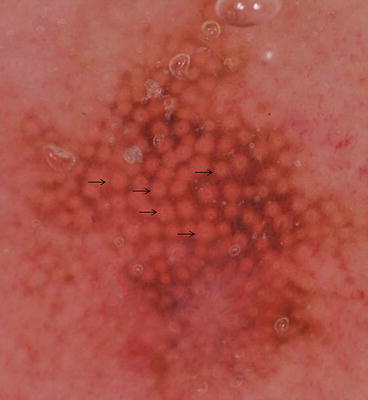
Fig. 4.4
Dermoscopy image of lentigo maligna melanoma on the earlobe showing pseudonetwork pattern and numerous circle-within-a-circles (arrows)

Fig. 4.5
Dermoscopy image of lentigo maligna melanoma on the cheek with many circle-within-a-circles (arrows)
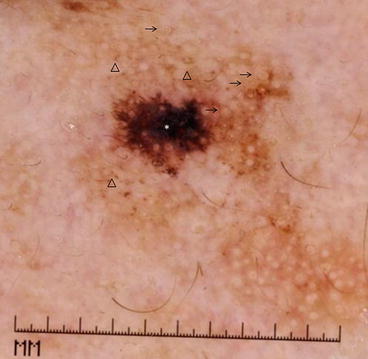
Fig. 4.6
Dermoscopy image of lentigo maligna melanoma on the cheek with asymmetrically pigmented follicular openings with granularity (triangles), circle-within-a-circles (arrows), and central blotch with obliteration of follicular openings and presence of blue-white veil (asterisk)
Grey dots/granules surrounding follicular openings. Gray dots/granules correspond on histopathology to melanophages in the upper dermis. Rarely one can also see streaks, which correspond to confluent junctional melanocytes [2, 11].
Annular-granular pattern created when both gray dots/granules surrounding follicular openings and asymmetric pigmented follicular openings are present [2, 8]. At times the dots can be larger, corresponding to nests of melanocytes, and then these structures are called globules.
Shiffner et al showed that the presence of asymmetrically pigmented follicular openings, gray dots, gray globules, or rhomboidal structures located anywhere within a lesion has a sensitivity of 89 % and a specificity of 96 % for LMM [2]. Pralong et al found that at least one of these structures is present in 87 % of LMMs [13]. The presence of gray color appears to be a useful clue to the diagnosis of LMM [14]. In a series of 201 LMMs, gray color was present in 88.6 % of cases [15]. Tschandl et al further reported that any gray structures, such as dots, circles, or lines, were present in 95.8 % of LMM lesions with a relative risk of 8.9 (95 % CI: 1.2–64.7) [16]. While gray color is possible in pigmented actinic keratosis and LPLK, this color is rare in solar lentigo and flat seborrheic keratosis.
Less prevalent dermoscopic features associated with LM/LMM include the isobar structure or the “circle-within-a-circle”, identified in 5 % and 25.4 % of cases in 2 separate series [15, 16]. More recently described features include red rhomboidal structures, increased lesional vascular network density, and target-like pattern [13]. Red rhomboidal structures are created by a diamond or rhomboid-shaped vascular pattern occurring between hair follicles, and were reported to be present in 40 % of cases [13]. An increased density of the vascular network within the lesion compared to the peripheral skin was found in 58 % of cases [13]. A target-like pattern, defined as a dark dot in the center of the dark circle of a hyper-pigmented hair follicle, has been found in 19.4 % and 41 % of cases [13, 15]. Finally, the perception of the degree of pigment present within a lesion is a clue to the diagnosis of LM/LMM. In 25 % of LM/LMM the pigment appears darker and more variegated with different shades of brown and gray when viewed with dermoscopy compared to naked-eye examination [13].
It is plausible that certain LM/LMM-specific features are related to the type/thickness of the melanoma, the anatomical location of the tumor, or to patient-specific phenotypic factors. For example, Tiodorovic-Zivkovic et al showed that rhomboidal structures are more frequently seen in LMM located on the upper part of the face (p = 0.028), whereas asymmetric follicular openings were more common in LMM located on the lower part of the face (p = 0.036) [15]. Table 4.1 summarizes frequency and diagnostic accuracy of dermoscopic features of LMM.
Table 4.1
Frequency and measures of diagnostic accuracy of dermoscopic features described for lentigo maligna melanoma
Authors | Dermoscopic Feature | Prevalence n, (%) | Sensitivity (%) | Specificity (%) |
|---|---|---|---|---|
Schiffner et al. [2] | Asymmetric follicular openings | 25/37 (68) | 67.6 | 88 |
Rhomboidal structures | 18/37 (49) | 48.6 | 100 | |
Asymmetrically pigmented follicular openings, Rhomboidal structures, Gray globules, Gray dots | 34/37 (93) | 89 | 96 | |
Pralong et al. [13] | Rhomboidal structures | 86/125 (69) | 68.8 | |
Pigmented follicular openings | 64/125 (51) | 51.2 | ||
Annular-granular pattern | 53/125 (42) | 42.4 | ||
Obliterated hair follicles | 16/125 (13) | 12.8 | ||
Circles and semicircles | 59/125 (47) | 47.2 | ||
Circle-within-a-circle | 6/125 (5) | 4.8 | ||
Target like pattern | 51/125 (41) | 40.8 | ||
Red rhomboidal structures | 50/125 (40) | 40.8 | ||
Tschandl et al. [16] | Any gray structure | 23/24 (96) | 95.8 | 30.6 |
Gray dots, clods, circles or lines | 13/24 (54) | 54.2 | 83.3 | |
Circle-within-a-circle | 1/24 (4) | 4.2 | 98.1 | |
Rhomboidal structures | 4/24 (17) | 16.7 | 91.7 | |
Tiodorovic- Zivkovic et al. [15] | Gray color | 178/201 (89) | 88.5 | |
Asymmetric follicular openings | 89/201 (44) | 44.3 | ||
Annular Granular pattern | 55/201 (27) | 27.4 | ||
Circle-within-a-circle | 51/201 (25) | 25.4 | ||
Rhomboidal structures | 36/201 (18) | 17.9 | ||
Obliterated hair follicles | 25/201 (12) | 12.4 | ||
Target like pattern | 39/201 (19) | 19.4 | ||
Red rhomboidal structures | 4/201 (2) | 2 | ||
Jaimes et al.a [10] | Patchy peripheral pigmented islands | 28/76 (37) | 36.8 | |
Angulated lines pattern | 23/76 (30) | 30.3
Related posts: Epidemiology and Natural History Epidemiology and Natural History
 Incorporating Patient Preferences and Quality of Life Incorporating Patient Preferences and Quality of Life
 Case B: Unsuspected Invasion and Upstaging in Lentigo Maligna Melanoma Case B: Unsuspected Invasion and Upstaging in Lentigo Maligna Melanoma
 Staged Excision Techniques Staged Excision Techniques
 Follow Up and Recurrence Follow Up and Recurrence
 Case A: Multiple Mapping Techniques to Guide Staged Excision for a Challenging Lentigo Maligna Melanoma Case A: Multiple Mapping Techniques to Guide Staged Excision for a Challenging Lentigo Maligna Melanoma
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|