Right donor hepatectomy for live donor liver transplantation is the removal of segments 5, 6, 7, and 8 from a living donor for transplantation in a recipient with end-stage liver disease. This is the most commonly performed hepatectomy in living donors for the purpose of adult-to-adult living donor liver transplants in the United States.1 We describe a hybrid technique that incorporates laparoscopic mobilization of the liver that aids performing the operation through an upper midline incision.
PATIENT HISTORY AND PHYSICAL EXAMINATION
Patients who volunteer to become living donors should have extensive workup to assess their suitability for candidacy. This workup includes medical, physical, and psychosocial assessment of the donor. Additionally, donors undergo an assessment of the potential graft through evaluation of liver anatomy, volume, and function.
Donors should be between ages 20 and 60 years. A detailed history should specifically focus on the presence of any underlying hepatic disease, cardiovascular disease, respiratory disease, hypercoagulable states, bleeding disorders, malignancy, and abdominal surgeries.
A family history should also be elicited again focusing on the earlier.
A thorough physical exam should also be performed to assess for any underlying undetected cardiovascular issues, liver diseases, and previous abdominal surgeries.
Donors should meet with a physician not employed by the transplant center. This physician functions as an independent donor advocate ensuring medical and psychological appropriateness. Donors should also have an evaluation by a psychiatrist, social worker, and a financial counselor to ensure adequate emotional and financial resources to handle the donation and possible complications.
Table 1: List of Laboratory Tests Performed in all Potential Living Liver Donors
Comprehensive laboratory tests are performed on potential living donors (Table 1). This includes an assessment for occult liver disease including hepatitis B and C, α1-antitrypsin disease, hemochromatosis, primary biliary cirrhosis (PBC), and autoimmune hepatitis (AIH).
Potential donors undergo laboratory workup to exclude underlying procoagulant disorders.
Additionally, common cancer markers are also sent to exclude the potential of occult malignancy; these include a prostate-specific antigen (PSA) (in men), carcinoembryonic antigen (CEA), and α-fetoprotein.
A full toxicology screen is performed as part of the evaluation, and a pregnancy test is sent on female patients of childbearing age.
The vasculature and biliary anatomy of the liver are evaluated with computed tomography angiography (CTA) or magnetic resonance imaging (MRI) or magnetic resonance cholangiopancreatography (MRCP). These imaging modalities are also used to assess liver volumes with the aid of computer software designed specifically for this purpose. MRI techniques that can estimate hepatic steatosis are used.2 Preoperative imaging should clearly show the hepatic arteries, portal veins, hepatic veins, and biliary tree to at least third-order branches.
SURGICAL MANAGEMENT
Preoperative Planning
For patients with Model for End-Stage Liver Disease (MELD) greater than 18, we accept donors whose grafts will give a graft-to-recipient weight ratio (GRWR) of greater than 0.8. For recipients with MELD less than 18, we accept a GRWR less than 0.8 and greater than 0.5. The average right lobe graft in the United States is 966 g,1 enabling GRWR of greater than 0.8 for recipients up to 120 kg.
Donors with remnant liver volume of less than 30% of total liver volume are excluded from donation. Relative anatomic contraindications include more than two bile ducts draining the right lobe, right posterior bile duct draining into the left bile duct, and left portal vein arising from right anterior portal vein. Donors with greater than 30% macrosteatosis are excluded from donation.
Recipients with portal vein thrombosis should be carefully evaluated with MRI or magnetic resonance venography (MRV) or three-phase computed tomography (CT) to determine the level of the thrombosis and need for additional vessels. Because the living donor portal vein is shorter than deceased donor, recipients with portal vein thrombosis may require jugular vein grafts or be excluded from living donor liver transplant.
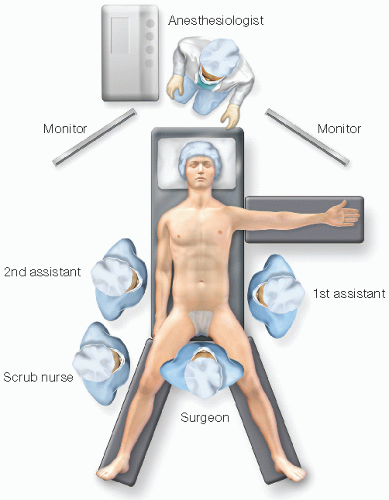
FIG 1 • Patient position.
The donor and recipient teams should meet in advance to discuss technical issues with both the donor and recipient operations.
Patient Preparation and Positioning
Donors are given 5,000 units of subcutaneous heparin prior to induction.
Two large-bore intravenous lines are placed, as well as an arterial line, to allow continuous blood pressure monitoring. Central venous catheters are not needed.
Once intubated, place a Foley catheter and place the patient in the supine position on a split leg table with the right arm tucked (FIG 1). This aids the positioning of the surgeon for the laparoscopic portion of the operation.
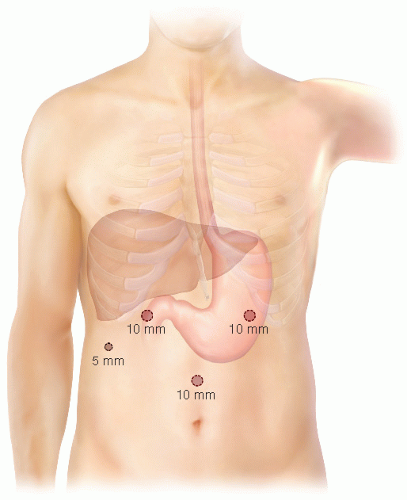
Place the ports as shown in FIG 2, and move the patient into the reverse Trendelenburg position.
FIG 2 • Port placement.
TECHNIQUES
LAPAROSCOPIC MOBILIZATION OF LIVER
Use a LigaSure device (Valleylab), a Harmonic scalpel, and a monopolar cautery energy device for the laparoscopic portion of the procedure.
Begin the mobilization by taking down the falciform ligament using the LigaSure and Harmonic scalpel. Transect the falciform posteriorly to the hepatic veins.
Dissect the areolar tissue overlying the hepatic veins using the scissors and a combination of sharp dissection and monopolar cautery. Continue the dissection to expose all three hepatic veins.
Mobilize the right triangular ligament to clearly expose the right hepatic vein. This is achieved through careful sharp dissection of the triangular ligament and diaphragm. Care must be taken not to injure the vein or the surrounding phrenic veins.
Turn attention to the hepatorenal ligament. Make an 8-cm incision 3 to 5 cm above the supraumbilical port and place a GelPort (Applied Medical) into the abdomen. The assistant elevates the liver using their left hand, exposing the hepatorenal ligament (FIG 3A).
Only gold members can continue reading. Log In or Register to continue