Rib Cartilage
Cartilage is a bradytrophic tissue (scant blood supply) and, as such, is excellent for reconstruction and augmentation of the trachea, nose, cheek, skin, and ear (Weerda 1985a).
Obtaining Rib Cartilage for Ear Reconstruction
( Fig. 11.1 )
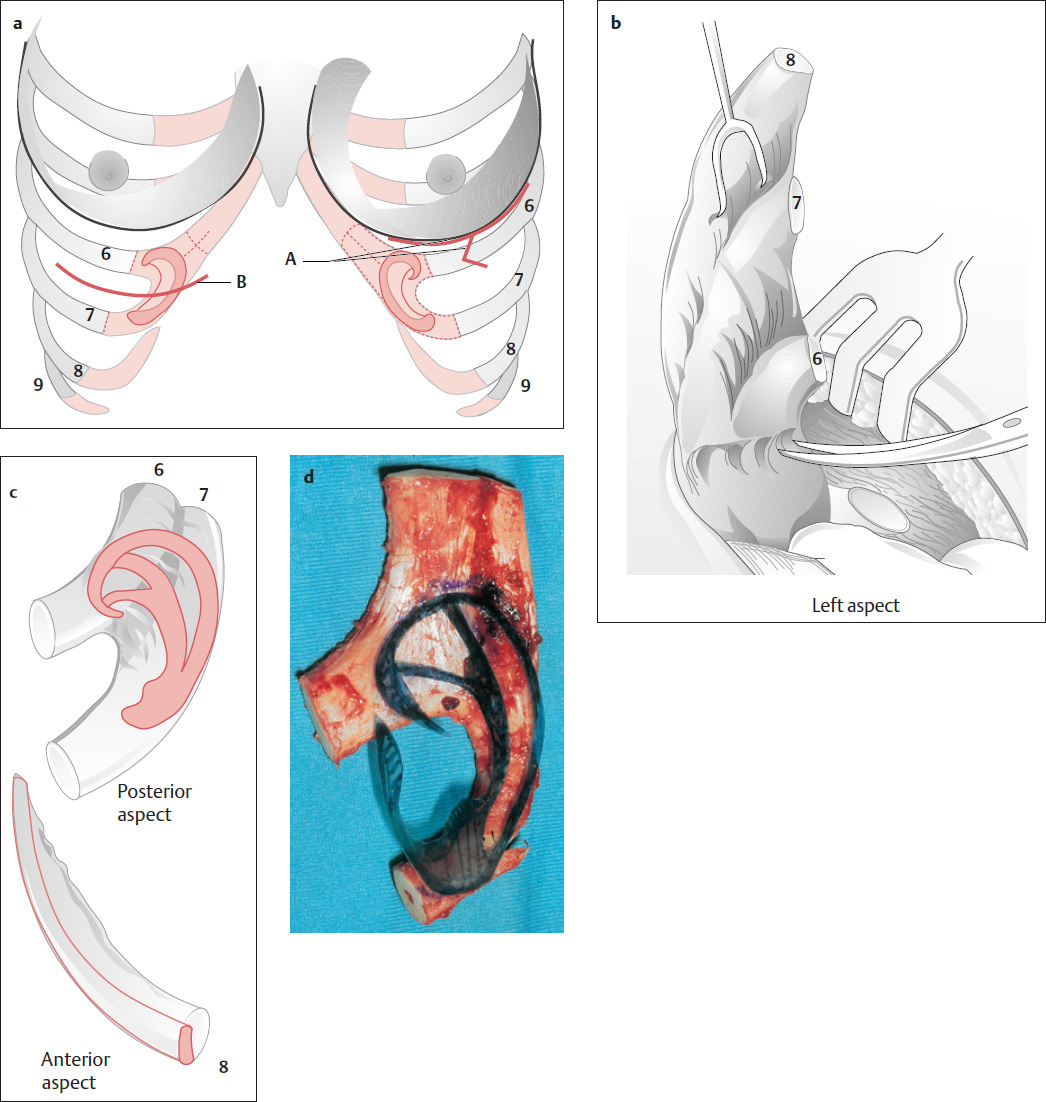
Rib cartilage is generally obtained from the same side of the thorax, under general anesthesia. Small amounts of cartilage can be taken from the fourth, fifth, or sixth rib, close to the sternum. We usually incise along the inframammary fold in women ( Fig. 11.1a , A) and parallel to the donor site in men ( Fig. 11.1a , B). The seventh rib is the longest cartilaginous rib and the last rib that extends to the sternum. The eighth rib is somewhat shorter and is often connected to the seventh rib by a synchondrosis. The sixth and seventh ribs generally supply a sufficient block to carve the body of the auricular framework ( Figs. 11.1 and 11.3 ). The eighth rib can be used to make the helical rim, if it is at least 8 cm long (preferably 9–10 cm).
Operative Technique
We usually anesthetize the incision site with a local anesthetic solution containing epinephrine (diluted 1:200,000). The skin is incised parallel to the rib, or over the costal arch (eighth rib), and all layers are divided down to the rib. Attention is given to the pleura, which should remain intact if at all possible. When whole cartilaginous ribs are removed, the muscle is cut close to the cartilage with an electrocautery device, or the perichondrium is dissected from the cartilage surface. If pleural injury occurs (under general anesthesia), a small piece of fascia (free or pedicled) should be glued over the defect and the wound closed over a suction drain while ventilation is maintained. With a small wound in the parietal pleura, and an airtight layered closure, there should be no further difficulties. The fascial and subcutaneous layers should be closed separately. We generally use 4-0 (or 3-0) intracutaneous monofilament sutures for skin closure (see Fig. 2.5 ).
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


