Procedural sedation for a rhinoplasty, like any procedure, relies on careful patient selection and patient and surgeon compliance. Patients should have an American Society of Anesthesia (ASA) score of 1 or 2, with a possibly well-controlled 3 also acceptable, and should be devoid of certain comorbidities, including obstructive sleep apnea, gastroesophageal reflux disease, and obesity (body mass index ≥35). Before the procedure begins, clinicians must explicitly communicate to patients that they will feel no pain; however, because they are being sedated, they may know what is occurring during surgery, but they should not care. A common misconception about sedation is that it involves general anesthesia without an airway. Clinicians must reassure patients that the anesthetist will be with them the entire time, and any discomfort can be dealt with immediately and the anesthesia titrated to an acceptable level.
Key points
- •
Procedural sedation for rhinoplasty is best achieved with combination local anesthesia and systemic pharmacology.
- •
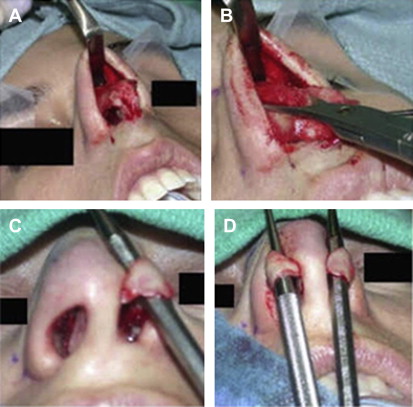
In our practice, 80% of rhinoplasty is performed via a closed technique with a cartilage delivery approach to address the nasal tip.
- •
General anesthesia is used at the patient’s request and for long and difficult cases.
Sedation for rhinoplasty
Procedural sedation for a rhinoplasty, like any procedure, relies on careful patient selection and patient and surgeon compliance ( Fig. 1 ). Patients should have an American Society of Anesthesia (ASA) score of 1 or 2, with a possibly well-controlled 3 also acceptable, and should be devoid of certain comorbidities, including obstructive sleep apnea, gastroesophageal reflux disease, and obesity (body mass index ≥35).
Before the procedure begins, clinicians must explicitly communicate to patients that they will feel no pain; however, because they are being sedated, they may know what is occurring at the time of surgery. A common misconception about sedation is that it involves general anesthesia without an airway. Clinicians must reassure patients that the anesthetist will be with them the entire time, and any discomfort can be dealt with immediately and the anesthesia titrated to an acceptable level.
Anesthetic technique
For the actual anesthetic technique, given that this is an anesthetic for airway surgery with a shared airway with the surgeon, certain goals must be maintained at all times.
- •
Immediate access to the airway is not always accessible, thus the level of sedation must be on a plane of anesthesia that allows the patient to maintain their oxygen saturation, hemodynamics, and airway reflexes to prevent aspiration of blood and gastric contents.
- •
Like any anesthetic, nothing-by-mouth guidelines as per the ASA must be met before the procedure is started.
Anesthesia can be administered in multiple ways. This article provides insight into the authors’ technique; however, each anesthetic must be tapered to the individual needs of the surgeon, patient, and anesthesiologist.
- 1.
The procedure begins with preoxygenation through a facemask delivering a minimum of 8 liters per minute of oxygen. The standard monitors are applied to the patient (eg, noninvasive blood pressure amplifier, electrocardiogram, pulse oximeter).
- 2.
Through a free-flowing intravenous tube connected to saline or lactated Ringer solution, a cocktail is injected consisting of the following:
- •
Anxiolytic medication, such as a benzodiazepine (2–3 mg of midazolam)
- •
Short-acting narcotic (50–100 μg of fentanyl)
- •
An antinausea medication with sedative properties (diphenhydramine, 50 mg)
- •
This injection provides the baseline sedation for the procedure. Subsequently, every 30 to 60 minutes, depending on the level of the patient’s sedation, the authors “top-up” with 1 mg of midazolam and 50 μg of fentanyl for the duration of the case.
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


