Reversed Superficial Temporal Artery Postauricular Compound Skin and Cartilage Flap
M. ORTICOCHEA
EDITORIAL COMMENT
The principle of reversal of flood described in this chapter, both arterial and venous, has taken on considerable importance over the past several years, both in this and other sites of the body. The innovative technique of nasal reconstruction is a relatively complicated one, and the goal might be achieved more simply with some of the other techniques described.
The three anatomic structures of skin coverage, nasal framework, and nasal lining can be found in the external ear. The retroauricular skin and that of the mastoid region will cover the nasal surface. The conchal cartilage and, occasionally, a long, thin portion of the mastoid and temporal bone will provide the framework. The thin skin firmly adhering to and covering the lateral surface of the cartilage of the conchal cavity will form the internal lining of the reconstructed nose.
INDICATIONS
Bilateral reversed superficial temporal artery postauricular compound skin and cartilage flaps can be used for total nasal reconstruction (1, 2, 3, 4). The advantages are that coverage, lining, and framework can be provided at the same time. The skin is the same color, texture, and thickness as that of a normal nose. The patient can breathe normally, since the nostrils are of a good size.
The ears from which the conchae have been removed keep their normal shape, size, and appearance and are only slightly flatter than normal. Replacement of the concha by a skin graft does not change its cosmetic appearance.
ANATOMY
The technique depends on the transfer of each concha on a flap with its base on the temple and including the superficial temporal vessels. To make this feasible, the natural flow of blood in these vessels must be reversed.
This is accomplished by dividing the vessels in front of the ear and transplanting the cut end into the substance of the flap behind the ear (see Fig. 59.4). The retrograde blood supply then comes from the natural anastomoses with the branches of the ophthalmic vessels in the lateral forehead (supraorbital, supratrochlear, and lacrimal).
This principle of reversal of blood flow is applicable to many flaps in facial and body reconstruction and makes new flap designs possible.
FLAP DESIGN AND DIMENSIONS
The flap base must be fairly high in the frontal area to ensure sufficient flap length. Otherwise, there may be difficulty in bringing the concha far enough to reconstruct the alae, nostrils, and columella. Vascular impairment of the upper pole of the remaining portion of the ear may occur if the crus of the helix pedicle is too narrow. It is important to include all the skin adjacent to the triangular fossa with the pedicle. Postoperative edema of the reconstructed nose may persist for some months, but later resolves. Tissue contraction occurs postoperatively at all stages. For this reason, all the postauricular skin is included in the flap. Hairy skin, however, is avoided.
OPERATIVE TECHNIQUE
Total nasal reconstruction using this technique requires four stages:
The flaps are delayed on each side of the head.
The lower pedicle of each flap is delayed (see Fig. 59.6).
The auricular ends of the flaps are sutured to their new site in the nasal region (see Fig. 59.7).
The carrier pedicles are returned to their donor sites, and any revisions of the new nose are carried out (see Fig. 59.8).
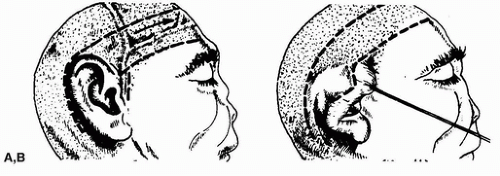 FIGURE 59.1 A: The flap is 4 cm wide and it overlies the superficial temporal vessels. The preauricular incision allows exposure of the vessels, which are ligated at the level of the tragus and subsequently transplanted beneath the flap. B: On the posterior ear, the incision is made 1 cm from the helical rim. (From Orticochea, ref. 4, with permission.) |
Stage 1
The patient is placed in the Trendelenburg position to engorge the superficial temporal vessels, and the flaps that overlie these vessels are marked. Each flap measures 4 × 12 cm (Figs. 59.1 and 59.2). The patient is returned to the Fowler position before the flaps are incised.
Related posts:
 Cheek Rotation Skin (Mustardé) Flap to The Lower Eyelid
Cheek Rotation Skin (Mustardé) Flap to The Lower Eyelid
 Nasalis Musculocutaneous Sliding Flaps for Nasal Tip Reconstruction
Nasalis Musculocutaneous Sliding Flaps for Nasal Tip Reconstruction
 Oral Mucosal Flaps for Septal Reconstruction
Oral Mucosal Flaps for Septal Reconstruction
 Postauricular and Retroauricular Scalping Flap (The Paras Flap)
Postauricular and Retroauricular Scalping Flap (The Paras Flap)
 Scapular and Parascapular Flaps
Scapular and Parascapular Flaps
 Platysma Musculocutaneous Flap to The Lower Lip
Platysma Musculocutaneous Flap to The Lower Lip
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


