Reverse Flow Radial Forearm Flap
Kate Elzinga
Kevin C. Chung
DEFINITION
The most commonly used regional flap for coverage of volar and dorsal hand and wrist wounds is the reverse radial forearm flap (RRFF). It is a reliable and versatile flap.
The radial forearm flap can be used as an antegrade flap to cover defects of the elbow.
The radial forearm flap can also be harvested as a free flap for distant defects.
The RRFF can be designed up to 35 × 15 cm in size, harvesting up to two-thirds of the circumference of the forearm, from 4 cm distal to the antecubital fossa to the wrist crease.
The RRFF’s large size makes it suitable for coverage of nearly all wrist and hand wounds. However, the arc of rotation of the flap into the defect typically precludes harvesting the flap extending to the distal forearm.
The flap can be pre-expanded to further increase its dimensions proximally in the forearm for adequate use as a reverse flap, although this is rarely necessary.1
ANATOMY
The RRFF is a Mathes and Nahai type B flap; it is supplied by septocutaneous perforators. Its pedicle is the radial artery and its two accompanying vena comitantes. The radial artery is divided proximally. Retrograde flow occurs from the ulnar artery through the deep palmar arch into the radial artery to provide arterial inflow to the flap.
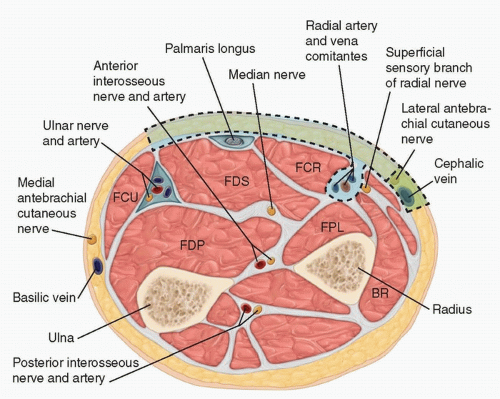
FIG 1 • The radial artery and its vena comitantes are found in the distal forearm within the intermuscular septum between the BR radially and the FCR ulnarly. The radial border of the RRFF can be centered over the radial artery as shown here. Alternatively, the flap can be designed with its radial margin over the radial artery. The LABC and cephalic vein are optional structures that can be included in the flap design.
The radial artery originates from the brachial artery. It travels under the brachioradialis (BR) for most of its course. Distally, it is found in the interval between the BR radially and the flexor carpi radialis (FCR) ulnarly. The radial artery perforators travel within the septum between the BR and FCR to supply the overlying fascia and skin (FIG 1).
There are 6 to 10 septocutaneous perforators arising from the radial artery 2 cm proximal to the radial styloid.2 A reverse radial artery perforator flap can be elevated on these perforators to preserve the radial artery for patients without an intact palmar arch.3,4
The cephalic vein can be harvested with the RRFF although it does not play a role in the venous drainage of reverse flaps. Venous outflow is through the avalvular oscillating veins.5 In cases of venous congestion, anastomosis of the cephalic vein within the flap will decompress the venous congestion.
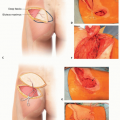
The RRFF is designed over the proximal and middle volar forearm.
The RRFF can be harvested as a fasciocutaneous, adipofascial, or fascia-only flap. It may also be raised above the fascia; the subcutaneous tissue and dermis above the fascia are raised suprafascially.
The lateral antebrachial cutaneous nerve (LABC) can be harvested with the flap and coapted to a sensory nerve at the defect site to innervate the flap.
Alternatively, the LABC can be left in situ during flap harvest, preserving the sensation to the radial forearm.6
The palmaris longus can be elevated with the flap for use as a vascularized tendon graft. For example, it can be used for an extensor tendon defect or to create a flexor pollicis longus during osteoplastic thumb reconstruction with an iliac crest bone graft and a RRFF.7 The BR can also be included as a vascularized tendon graft or part of the radius as a vascularized bone graft.8
The pivot point for the RRFF is the radial styloid.
PATIENT HISTORY AND PHYSICAL FINDINGS
The patient is assessed for suitability for regional flap reconstruction following a wrist or hand injury.
Important history includes the patient’s age, handedness, and occupation and avocations.
The patient’s past medical history, medications, allergies, and social history are noted. In particular, risk factors for flap loss, poor wound healing, and additional postoperative complications are discussed.
Comorbidities associated with poor wound healing include smoking, diabetes mellitus, end-stage renal disease, cardiac disease, peripheral vascular disease, vasculitis, malnutrition, immunosuppression, and hypercoagulable states.
Details of previous trauma or surgeries to the forearm are gathered. History of any previous radial artery cannulation for invasive blood pressure monitoring is also important.
If there is concern of damage to the radial artery or its perforators, angiography can be performed to evaluate the vascularity of the arm.
The patient’s defect is examined. The size of the wound is measured. Exposed structures, necrotic tissues, and any signs of infection are documented.
Wounds with exposed tendon and bone are best covered using flaps. The radial forearm flap is a pedicled regional flap that can be safely performed in most patients. It alleviates the need for a two-stage flap reconstruction such as a groin flap or microvascular reconstruction with a free flap.
The vascularity of the hand must be carefully assessed. If the radial artery is harvested for the RRFF, the patient must have an intact palmar arch with arterial inflow from the ulnar artery to prevent hand and finger ischemia.
The modified Allen test is used to clinically assess the integrity of the palmar arch (FIG 2). The examiner compresses the patient’s ulnar and radial arteries at the volar wrist and then instructs the patient to open and close the hand into a tight fist until the palm is blanched. The examiner then releases the ulnar artery and looks for arterial flow from the ulnar artery through the palmar arch to the radial side of the hand within 6 seconds. The test is repeated to assess the radial artery.
The motor and sensory nerves of the hand and forearm are tested. Any pre-existing abnormalities are noted.
IMAGING
Plain radiographs are performed for patients with traumatic wounds. Any fractures, foreign bodies, and abnormal joint intervals secondary to ligamentous injuries are noted.
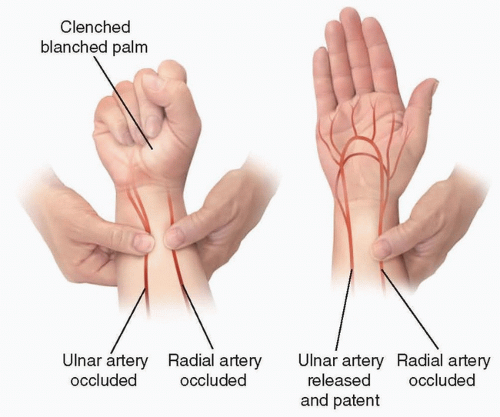
FIG 2 • The modified Allen test is used to confirm retrograde flow into the radial artery from the ulnar artery across the palmar arch prior to division of the radial artery for a RRFF. If the palmar arch is not patent, a reverse radial artery perforator flap or alternate flap should be used instead.Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree

 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access