Repair of Lip Commissure Defects With Estlander Flaps
Simon G. Talbot
Julian J. Pribaz
DEFINITION
Defects of the lips may occur from malignancy (most frequently squamous cell carcinoma followed by basal cell carcinoma), trauma, vascular malformations, or infections.1
There is disagreement in the literature about terminology.
Here, we refer to a lip switch flap not involving the commissure (either lower to upper lip as originally described or vice versa) as an Abbe flap.
We refer to a lip switch involving the commissure (either upper to lower or vice versa, as both were described in the original paper) as an Estlander flap.
We have chosen to not use the terms “reverse Abbe” and or “Abbe-Estlander,” which are sometimes used elsewhere to refer to upper to lower flaps excluding the commissure.
ANATOMY1
The lips include multiple layers of tissue: skin/subcutis, muscle, submucosa, and mucosa.
The vermilion forms a wide boundary between the mucosa and skin. Meticulous repair of the white roll (the external border of the vermilion and skin) is critical as defects in this border are easily noticed.
Lip function is controlled by the orbicularis oris muscles (sphincteric function) and numerous muscles of facial expression (elevation and depression functions).
Elevators include levator labii superioris, levator anguli oris, zygomaticus major and minor, levator anguli superioris, and mentalis muscles.
Depressors include depressor anguli oris, depressor labii inferioris, and platysma muscles.
Key external landmarks of the lips include Cupid’s bow, the philtral columns, the central tubercle, the white roll, and the commissure.
Arterial supply is through the facial artery branching into the superior and inferior labial arteries. These run just deep to the mucosa in the submucosal layer just deep to the orbicularis oris muscle, at the level of the mucosal-vermilion junction (FIG 1).
Venous drainage does not follow the arterial pattern, but a dense plexus exists in the lips.
Sensation is supplied by the infraorbital branch (upper lip) and mental branch (lower lip) of the trigeminal nerve.
Motor function to the orbicularis oris is supplied by the buccal branches of the facial nerve.
Additional muscles of facial expression are supplied by the zygomatic and mandibular branches.
PATIENT HISTORY AND PHYSICAL FINDINGS
Because of the unique anatomy and appearance of the lips, when defects involving the lips are too large to close directly, local flaps using the similar-appearing “like tissue” from the opposite lip are ideal.
Estlander flaps are suited for patients presenting with a fullthickness defect of the lateral lip up to and including the commissure.
Defects up to a quarter of the upper lip and one-third of the lower lip can usually be closed directly.
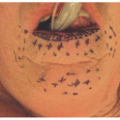
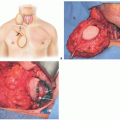
Flap closure is more appropriate for defects of half to three-quarters of the upper or lower lip (FIG 2).
Larger defects may require additional or distant flaps.
Similar to an Abbe flap, the Estlander flap is a cross-lip flap. However, whereas the Abbe flap can rotate clockwise or anticlockwise based on either labial artery, the Estlander flap rotates around the commissure and can be based only on the contralateral labial artery as the ipsilateral vessel has usually been removed with the tumor extirpation.
A second-stage procedure to divide and inset the flap and reestablish the commissure is required, and this can be safely done at 3 to 4 weeks.
Estlander flaps can be used to reconstruct either upper or lower lip defects.2
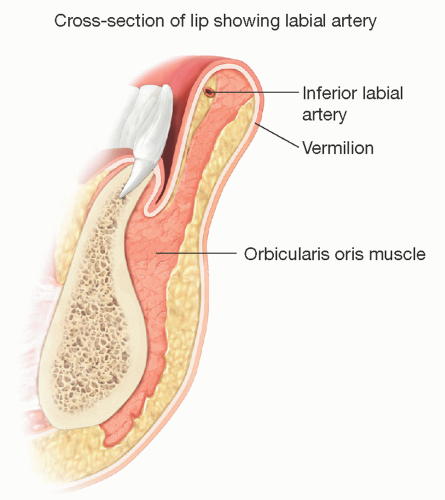 FIG 1 Cross-sectional anatomy of lower lip. |
 FIG 2 • Defect after Mohs resection of infiltrating basal cell carcinoma.
Related posts: Mandible Reconstruction With Fibula Flap With Templates Mandible Reconstruction With Fibula Flap With Templates
 Repair of Lip Defects With Karapandzic Flaps Repair of Lip Defects With Karapandzic Flaps
 Lower Eyelid Reconstruction With Palatal Grafts Lower Eyelid Reconstruction With Palatal Grafts
 Reconstruction of the Ear Lobe Reconstruction of the Ear Lobe
 Pectoralis Major Flap for Pharyngeal Reconstruction Pectoralis Major Flap for Pharyngeal Reconstruction
 Facial Reanimation in the Oncologic Patient Using Nerve Grafts and Nerve Transfers Facial Reanimation in the Oncologic Patient Using Nerve Grafts and Nerve Transfers
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|