Rectus Femoris Flap for Abdominal Wall Reconstruction
Alexander F. Mericli
Charles E. Butler
DEFINITION
The rectus femoris muscle can be used as pedicled or free flap for reconstruction of the abdominal wall.
The flap can be harvested as a myocutaneous or muscleonly flap, depending on the requirements of the defect.1,2,3,4
Several authors have had success employing the flap in an innervated fashion for abdominal defects.5
Depending on the size of the defect, the rectus femoris muscle can be designed as an isolated flap or can be combined with other components of the lateral femoral circumflex vascular axis (vastus lateralis, anterolateral thigh skin and subcutaneous tissue, iliotibial band, and/or tensor fascia lata muscle) for the creation of a subtotal thigh flap.1 For massive abdominal wall defects, bilateral flaps can be raised.
As a rotational flap, the rectus femoris muscle will easily reach the lower abdomen, mons, lateral hip, perineum, and groin.
Although the rectus femoris is recognized as a useful flap, debate continues regarding its associated donor-site morbidity.
ANATOMY
The rectus femoris is part of the quadriceps muscle complex. It is a bipennate muscle with two distinct muscle bellies (FIG 1A).
It has two separate origins: the anteroinferior iliac spine and the anterior rim of the acetabulum. The muscle inserts onto the patella along with the other components of the quadriceps complex and both flexes the hip and extends the knee (FIG 1B).
The motor innervation comes from the femoral nerve (L4 nerve root). The sensory innervation to the skin overlying the muscle is from the intermediate femoral cutaneous nerve.
The vascular supply of the rectus femoris is consistent with that of a type 2 muscle flap, as defined by Mathes and Nahai.
The major pedicle is a medial branch from the lateral femoral circumflex artery (FIG 1C). The branch to the rectus femoris muscle emerges 1 to 2.5 cm distal to where the lateral femoral circumflex artery splits from the profunda femoris artery. The pedicle tends to enter the muscle on its deep and lateral surface. After sending a branch to the rectus femoris muscle, the lateral femoral circumflex neurovascular bundle continues inferiorly, traveling in the septum between the vastus lateralis and rectus femoris muscle, to supply the tissue of the anterolateral thigh flap.
The minor pedicles are one to three small branches from the superficial femoral artery, distally. Generally, the minor pedicles are not independently sufficient to support flap viability.
The muscle is bordered by the vastus medialis medially, the vastus lateralis laterally, and the vastus intermedius on its deep surface. The sartorius muscle crosses obliquely over the rectus femoris muscle proximally.
PATIENT HISTORY AND PHYSICAL FINDINGS
Since the advent of the component separation technique, fascial approximation of defects up to 20 cm wide at the umbilicus can be achieved. Therefore, autologous reconstruction of the abdominal wall using thigh-based flaps is reserved for patients with total or massive subtotal defects of the full thickness of the abdominal wall.
The etiology of these significant defects is variable and includes malignancy (tumor resection; FIG 2A), trauma (damage control of the abdomen or soft tissue loss due to ballistic or blunt injury), and infectious processes (necrotizing fasciitis, full-thickness abdominal wall resection due to extensive enterocutaneous fistula formation; FIG 2B,C).
IMAGING
Imaging studies are not required before performing a rectus abdominis flap for abdominal wall reconstruction. However, imaging is often present for other reasons and can be utilized to the reconstructive surgeon’s advantage.
Computed tomographic scans of the abdomen and pelvis can be utilized for visualization of the abdominal defect size and associated anatomy.
Computed tomographic angiography of the lower extremity— if present—can be used to confirm patency of the vascular pedicle (FIG 3).
SURGICAL MANAGEMENT
Preoperative Planning
The patient should be seen preoperatively where a full history should be obtained and physical examination should be performed.
Special attention should be paid to a past history of any abdominal, groin, or thigh surgeries or injuries.
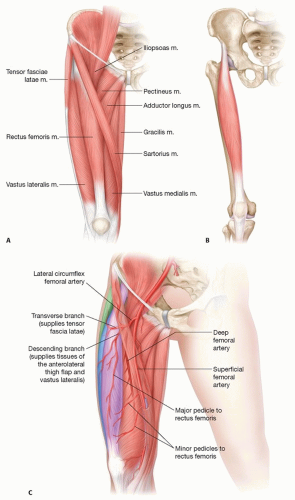
FIG 1 • A. Muscular anatomy of the thigh. B. The rectus femoris muscle originates from the anteroinferior iliac spine and the acetabulum. It spans both the hip and knee joints, thus serving as both a hip flexor and knee extensor. C. The rectus femoris muscle is supplied by the descending branch of the lateral femoral circumflex artery. The lateral femoral circumflex artery also supplies the tensor fascia lata, the vastus lateralis, and the overlying skin, allowing for a subtotal thigh flap to be designed, if necessary. Color code: rectus femoris muscle, purple; anterolateral thigh tissues, blue; tensor fascia lata, green.
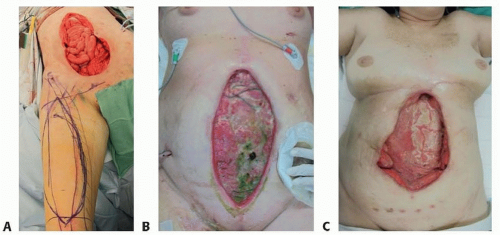
FIG 2 • Abdominal wall defects from various etiologies. Full-thickness defect after oncologic resection (A), enterocutaneous fistula and associated soft tissue loss after evisceration (B,C). (© Charles E. Butler, MD.)
If vascular disease is suspected, a computed tomographic angiogram should be considered to verify perfusion of the rectus femoris muscle.
Reconstruction of the abdominal wall is typically a multisurgeon case involving both reconstructive and general surgeons. General surgeons should be available to assist with adhesiolysis or any enteral repairs, which might be needed during the exposure.
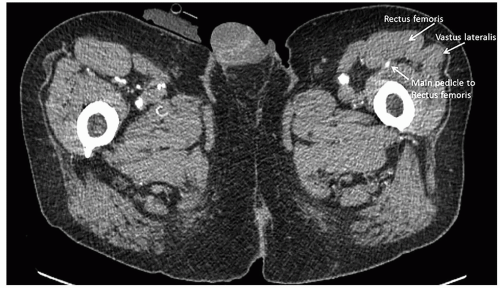 FIG 3 • Computed tomographic angiography demonstrating the cross-sectional anatomy of the thigh. |
Positioning
The patient is placed in the supine position with the bilateral legs internally rotated at the hip.
The legs are secured in this position at the forefoot with a combination of tape and foam to relieve pressure.
TECHNIQUES
▪ Markings
With the legs internally rotated, markings are placed on the anterosuperior iliac spine and the superolateral border of the patella; a line connecting these two points approximates the lateral border of the rectus femoris muscle.
A line is extended superiorly from the midpoint of the patella to the anterosuperior iliac spine representing the central axis of the rectus femoris muscle (TECH FIG 1).Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree