(1)
Division of Plastic-, Hand-, and Microsurgery Department of Surgery, Ludwig Maximilians University, Munich, Germany
6.1 Resection of Accumulated Fat via Liposuction Secondary to Lymphatic Flow Reconstruction
One of the sequels of diminished lymphatic transport which causes lymphedema is the surplus of fat tissue. In advanced forms improvement of lymphatic transport alone may not be sufficient for the patient if he strives for a normal appearance of the extremity. This is highly important in particular for arm edemas since it is more difficult to hide the upper than the lower extremities.
Reducing or eliminating the surplus of fat should be done with lymphatic vessel-sparing technique, if beforehand the lymphatic transport has been restored or at least improved by lymphatic vessel grafting.
In two studies we have examined the interaction between liposuction and the main lymphatic collectors.
It was shown that, at least under tumescence conditions, the danger to harm bigger lymphatic collectors is minimal (Frick et al. 1999, 2006; Hoffmann et al. 2004).
The anastomoses are located proximal to the area of edema. Mostly they are located at the upper part of the extremity. On the other hand, liposuction is performed within the edematous region distal to the anastomosing site. Therefore liposuction without damaging lymphatic anastomoses can be applied after reconstruction.
We perform it always after a time interval. Mostly after about 1 year. The patient can experience the result of the grafting and decide if he is satisfied with it. Mostly also the effect of the grafting is documented by a lymphoscintigraphy prior to secondary liposuction.
Up to now only in one patient a lymphatic grafting was performed as secondary procedure since the liposuction was performed earlier at another institution. The first liposuction has been performed according to our proposal of a lymph-sparing liposuction.
First experiences with nine patients suffering from secondary arm edemas have been published.
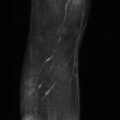
The preoperative mean volume of 3273 ± 292 cm3 was decreased to 2214 ± 149 cm3 after reconstructive surgery followed by liposuction. This was in the range of the normal contralateral arm with 2164 ± 140 cm 3 (P < 0.001) (Baumeister et al. 2007) (Fig. 6.1, Table 6.1).
Fig. 6.1
Results of the upper limbs
Table 6.1
Mean arm volumes prior to transplantation of lymphatic vessels compared to the volume after secondary liposuction
Lymphatic vessel transplantation (LTX) and secondary liposuction (SLS) in arm edema
Related posts: Pathophysiology of Lymphedemas with Respect to Surgery Pathophysiology of Lymphedemas with Respect to Surgery
 Methods for Objectification of the Results Methods for Objectification of the Results
 Experimental Basis of Reconstructive Lymph Vascular Surgery Experimental Basis of Reconstructive Lymph Vascular Surgery
 Indication and Technique of Reconstructive Lymph Vascular Surgery Indication and Technique of Reconstructive Lymph Vascular Surgery
 Results of Reconstructive Lymph Vascular Surgery Results of Reconstructive Lymph Vascular Surgery
 15: Hand Cleansers and Sanitizers 15: Hand Cleansers and Sanitizers
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|
|---|