Previous studies have shown large variation in the rate of common surgical procedures performed for the rheumatoid hand. This article provides a comprehensive overview of each surgical treatment option for rheumatoid hand reconstruction.
Rheumatoid arthritis (RA) affects the synovial tissue of the hand, resulting in the archetypal “rheumatoid hand” deformity. More than 70% of patients with RA complain of a loss in hand and wrist function, often restricting daily activities. This condition has a substantial societal effect in terms of growing treatment cost and productivity loss. Although surgical treatment can improve the quality of life for patients with rheumatoid hand, the indication for surgical intervention and the decision making among various treatment options are complex issues, for three main reasons.
First, RA is a polyarticular disease, and deformities in proximal joints will affect the position of the joints distally. Therefore the order of priority among necessary treatment steps must be considered and any proximal deformities first must be corrected. A patient presenting with destruction of the metacarpophalangeal joint (MCPJ) and proximal interphalangeal joint (PIPJ) may gain sufficient enough motion at the MCPJ after surgery that the need for surgery to correct the PIPJ is alleviated.
Second, the operative indication differs in each patient, which means an individual treatment plan must be formulated for each patient based on the status of the hand and the patient’s particular needs. For example, the presence of a hand deformity is not an absolute indication for surgery, because many patients maintain good function despite significant physical manifestation. Alternatively, patients may want the deformity corrected only to improve the appearance. A previous study by Alderman and colleagues using the Michigan Hand Outcomes Questionnaire showed that aesthetic consideration is a critical determinant of patient satisfaction in rheumatoid hand surgery.
Finally, rheumatologist and hand surgeons have different opinions regarding the indications, effectiveness, and outcomes of rheumatoid hand surgery. Most patients with RA are seen by rheumatologists who generally view rheumatoid hand surgery as a less effective remedy. Therefore, many patients with RA who are unresponsive to medication are still not referred for hand surgery consultation.
These complexities make a standardized strategy to treat the rheumatoid hand difficult to develop. Previous studies have shown a large variation in the surgical rates across the United States for common surgical procedures for the rheumatoid hand. The literature on treatment options and outcomes must be updated on a regular basis. The authors believe that this effort will help hand surgeons select proper treatment options tailored to each patient’s desired outcome. This article provides a comprehensive review of surgical treatment options for rheumatoid hand reconstruction.
Management of the rheumatoid hand
Wrist
Pathology
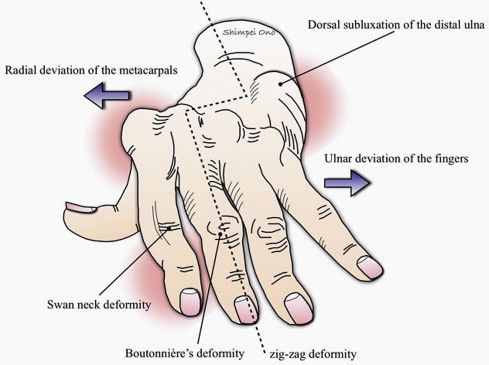
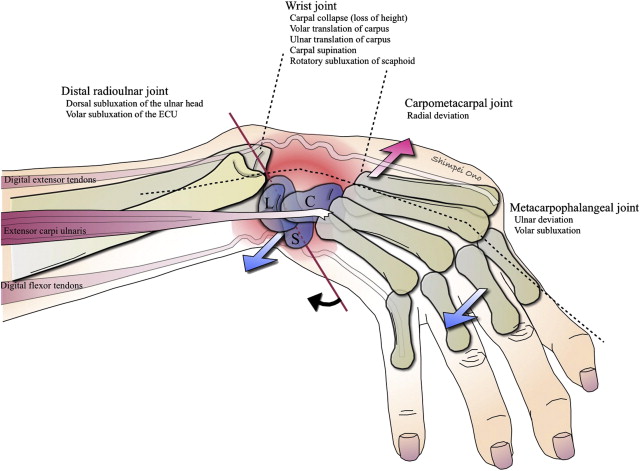
Dorsal subluxation of the ulnar head (or more precisely, volar subluxation of the radius because the ulna is a fixed unit of the forearm); supination, palmar and ulnar translation, and collapse of the carpus; and radial deviation of the carpometacarpal joint represent the deformities at the wrist ( Fig. 1 ). Synovitis often develops on the ulnar side of the wrist first. The synovial pannus progressively stretches the extensor carpi ulnaris (ECU) sheath and the capsuloligamentous apparatus of the distal radioulnar joint (DRUJ) and the radiocarpal, midcarpal, and carpometacarpal joints. Rupture of the ECU sheath results in palmar subluxation of the ECU. Furthermore, synovial proliferation within the DRUJ stretches the capsuloligamentous apparatus and eventually causes rupture of the triangular fibrocartilage complex (TFCC). With loss of the TFCC tether and the ECU restraint, the ulnar head dislocates dorsally, resulting in the classic caput ulnae. The palmarly subluxed ECU loses the ability to extend, and ulnarly deviates the hand. Along with the ECU, it becomes a wrist flexor and encourages palmar translation and supination of the carpus. The intact radial wrist extensors (extensor carpi radialis longus and extensor carpi radialis brevis) now act unopposed, causing the metacarpals to deviate radially. Degradation of the cartilage and interosseous cyst formation in the radius, scaphoid, and lunate, combined with radioscaphoid and midcarpal synovitis, leads to rupture of the scapholunate ligament, collapse of the scaphoid (scaphoid becoming horizontal with distal pole protruding into the carpal tunnel), bony destruction, and eventually carpal collapse. This loss in carpal height results in a relative lengthening of the flexor and extensor tendons and allows migration of the carpus toward the palmar and ulnar aspect of the radius (ulnar translation) ( Fig. 2 ). This movement is hastened by the natural inclination of the articular surface of the radius.
Roughly 75% of patients with RA show wrist symptoms, making it the most commonly affected joint in RA. During the early stages, patients develop wrist pain, tenderness, and bulging of the dorsal wrist. These symptoms may sometimes be alleviated through conservative treatment methods (eg, splinting). However, in advanced RA, several of the deformities described earlier may occur and restrict hand function through affecting the range of motion, grip strength, and overall function of the hand. The most commonly accepted indications of RA wrist surgery are when symptoms persist despite conservative treatment for at least 6 to 9 months, or when carpal deformity progresses. Surgical treatment is undertaken primarily to alleviate wrist pain or correct wrist deformities that affect the fingers. Surgery resulting in a stable and functional wrist is tantamount for the success of future hand reconstruction endeavors. Surgical options include synovectomy, excision of the distal ulna (Darrach procedure), fusion of the DRUJ (Sauve-Kapandji procedure), wrist arthrodesis, and arthroplasty.
Synovectomy
Wrist synovectomy ( Fig. 3 ) is usually recommended to treat refractory active synovitis or painful monoarthritis. However, the indications for it have never been clearly established. Lipscomb recommended several months of conservative therapy before performing a synovectomy, but Hindley and Stanley advocated early application of the procedure to prevent diseases progression. Ishikawa and colleagues found that synovectomy procedures can provide significant pain relief even in advanced cases of the disease. Controversy also exists regarding the effectiveness of wrist synovectomy. The benefits of wrist synovectomy are difficult to evaluate properly because the procedure is usually performed in conjunction with other surgical procedures. No studies currently show conclusively that a synovectomy can change the natural course of RA. Several authors have reported that during the early stages of RA, the procedure provides pain relief and maintains grip strength with a lower probability of tendon rupture but may cause varying degrees of long-term loss of wrist motion. Some investigators claim that the pain relief is ultimately transitory, with recurrence depending on the level of RA activity. Wrist synovectomy cannot stop the progression of intra-articular cartilage destruction completely.

Treatment of the DRUJ
Involvement of the DRUJ is a common cause of disability in the rheumatoid wrist, which may include wrist pain, restriction of pronation and supination, and compromised extensor tendons from a dorsally prominent ulnar head. Two procedures are commonly used to treat problems with the DRUJ.
Darrach procedure (distal ulna resection)
In 1912, Darrach first described resecting the distal ulna in a patient with anterior ulnar subluxation. This resection is followed by significant reduction of pain caused by DRUJ problems and ulnar impingement on the carpus. Its efficacy in preventing extensor carpi tendon rupture is unclear. This procedure is most commonly indicated in low-demand or elderly patients with persistent ulnar-sided wrist pain and limited forearm rotation caused by a DRUJ problem. Because forearm motion, grip strength, and lifting capability of the hand may be impaired, this procedure is usually not performed in high-demand patients. One concern with this procedure is the potential ulnar translation of the carpus in patients with weak ligamentous support. For patients whose lunates are already migrating toward the ulna, the Sauve-Kapandji procedure may be preferential, because the intact ulnar head can support the ulnar carpus. The other alternative would be to perform a concomitant radiolunate fusion alongside the Darrach procedure, provided that the midcarpal joint is intact. Combining the Darrach procedure with other surgical interventions is sometimes necessary to obtain optimal stabilization of the carpus. These treatment options may be possible for patients whose symptoms are limited to the radioulnar joint and whose radiocarpal joint is stable and functional.
Sauve-Kapandji procedure
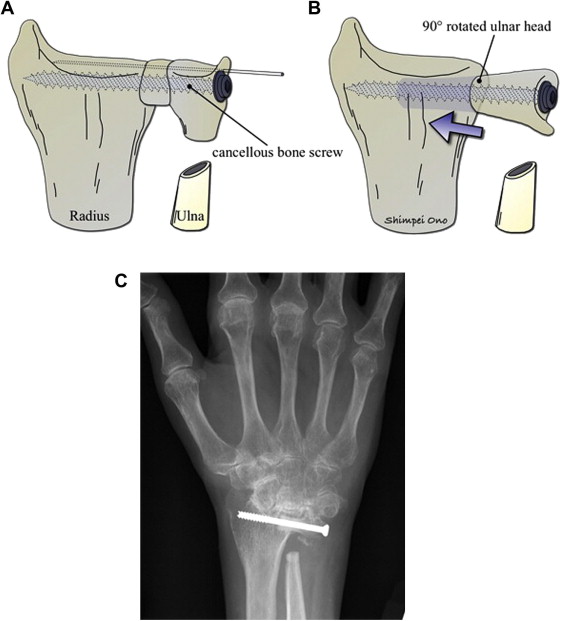
This procedure fuses the ulna head to the sigmoid notch of the radius and creates a pseudarthrosis by a proximal ulnar osteotomy to allow for rotation of the forearm ( Fig. 4 A). This procedure is more appropriate for younger or high-demand patients or those who have ulnar translocation of their carpus. A new joint is created farther down the ulna, stabilizing and preventing abnormal movement of the carpus at the DRUJ, while simultaneously unloading the ulna. This technique allows the ulna to be shortened, thereby transmitting more force across the radius rather than the damaged TFCC. Unfortunately, whether this method can prevent further dislocation of the carpus is still unclear, because robust studies on the long-term outcomes of the Sauve-Kapandji procedure are lacking. A potential problem is the unpredictable fusion of the DRUJ when the bone stock in RA is insufficient. Fujita and colleagues reported on the Modified Sauve-Kapandji procedure (see Fig. 4 B, C), which is designed to solve this problem. The modified procedure involves resecting the distal ulna and making a drill hole in the ulnar cortex of the distal part of the radius. The resected distal ulna is rotated 90°, inserted into the hole made in the distal radius, and secured with cancellous bone screw. The investigators concluded that the technique provides sufficient osseous support of the carpus in patients with poor bone quality.
Arthrodesis
For patients with symptoms arising from the radiocarpal joint, the choices are straightforward, involving either an arthrodesis or arthroplasty procedure. The arthrodesis procedures can be classified into either partial or total wrist fusion.
Partial wrist fusion
Partial wrist fusion is useful in patients with RA whose disease has destroyed the radiocarpal joints but has left the midcarpal joints unaffected. Limited arthrodesis of the involved joints combined with a synovectomy of the less-involved joints may relieve pain and preserve wrist motion. Radiolunate fusion, a representative of this kind of operation, was first described by Chamay and colleagues and is performed in addition to a synovectomy and ulnar head resection when ulnar translation of the carpus is seen on radiographs. A radiolunate fusion will stabilize the wrist and allow motion through the midcarpal joint. Reported results include a decrease in pain and prevention of further ulnar carpal translocation, thus allowing for a satisfactory level of joint mobility. Borisch and colleagues have shown long-term maintenance of the integrity of the midcarpal joint after radiolunate fusion.
Total wrist fusion
For patients with advanced arthritic changes in both the radiocarpal and midcarpal joints, total wrist fusion (TWF) is a well-established, safe, and reliable surgical option. TWF stabilizes the wrist and decreases pain, ultimately improving the patient’s quality of life. This procedure is sometimes selected as a salvage procedure after a previous wrist surgery has failed. TWF can be achieved successfully either using pins or plates. Several articles compare the efficacy of various arthrodesis techniques, but no significant difference in outcomes between techniques was observed.
Arthroplasty
Total wrist arthroplasty (TWA) is another motion-preserving alternative for patients with severe deformities. Unsolved problems exist related to joint replacement prostheses, including loosening of the prosthesis, implant fracture, periprosthetic bone problems, and degenerative wear of the implants. Therefore, choosing between performing a TWF or a TWA is sometimes difficult. A systematic review comparing TWF and TWA showed that outcomes of TWF procedures were potentially more appealing than those of TWA, but did not support the widespread application of TWA. Another decision analysis based on hand surgeon preferences assigned similar efficacies to TWF and TWA, showing that TWAs were only slightly preferred over TWFs. Moreover, an economic analysis showed that a TWA incurred only a slightly higher cost over the traditional TWF and that the incremental cost and quality-adjusted life-years for both treatment options were much lower than the acceptable range in the national criteria for adoption of a treatment strategy. Other studies attempting to determine superiority between the procedures have also remained inconclusive.
MCPJ
Pathology
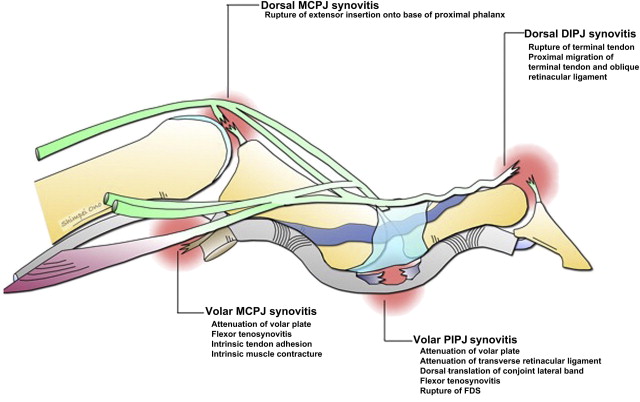
Palmar subluxation, ulnar deviation, and flexion represent the deformities seen at the MCPJ. The synovial pannus in the MCPJ stretches the joint capsule, leading to rupture of the extensor tendon insertion over the base of the proximal phalanx, and resulting in palmar subluxation of the proximal phalanx on the metacarpal head. Progressive synovitis leads to elongation and rupture of the collateral ligaments and the volar plate, which exacerbates the palmar subluxation of the proximal phalanx. The ulnar deviation deformity (see Fig. 1 ) results partly from the radial deviation of the metacarpals. The extensor tendons subluxate into the intermetacarpal sulcus, and this is aggravated by attenuation of the radial portion of the extensor hood. The flexor tendons also translate ulnarly because of stretching of the MCPJ capsule, and the vector generated by the pull of the flexor is oblique and ulnar in relation to the axis of the A1 pulley. The relative lengthening of the flexor and extensor tendons secondary to carpal collapse leads to unopposed action of the intrinsics, resulting in a flexion deformity at the MCPJ. Over time, this results in intrinsic contracture. Fine pinch function also becomes disordered from ulnar drift because the index and long fingers can no longer oppose the thumb in a tip-to-tip pinch.
In the early stages of rheumatoid MCPJ disease, synovectomy sometimes combined with a crossed intrinsic transfer is sufficient. For a patient with chronic MCPJ subluxation or joint destruction, soft tissue reconstruction will not be effective and an arthroplasty procedure will be necessary. In patients who have collapsed wrists and radial deviation of the metacarpals, the wrist should be addressed first; otherwise radial deviation of the metacarpals will cause early postoperative ulnar subluxation of the fingers after MCPJ arthroplasty. Finger MCPJ should not be fused unless arthroplasty is not possible, because fusion causes considerable functional impairment. Patients’ aesthetic consideration must be kept in mind, because the appearance of MCPJ is a prominent feature of the hand and shown to be important for men and women.
Synovectomy
Before considering a synovectomy, the patient must have an adequate amount of conservative therapy, including systemic medication, splinting, and local intra-articular corticosteroid injections. Synovectomies are indicated for patients with resistance to medical treatment, persistent MCPJ synovitis, minimal joint deformity, and minimal radiographic manifestations of RA. Intermittent painful synovitis is an additional indication for a synovectomy. Although the available data do not indicate an interruption or a decrease in disease progression, a significant reduction of pain is generally achieved. Sekiya and colleagues recently reported two case series regarding the usefulness of synovectomy procedures performed through arthroscopy of MCPJ and PIPJ in patients with RA. A recurrence of symptoms after the procedure is possible (30%–50% of patients undergo spontaneous remission), making the effectiveness of synovectomy procedures difficult to evaluate.
Crossed intrinsic transfer
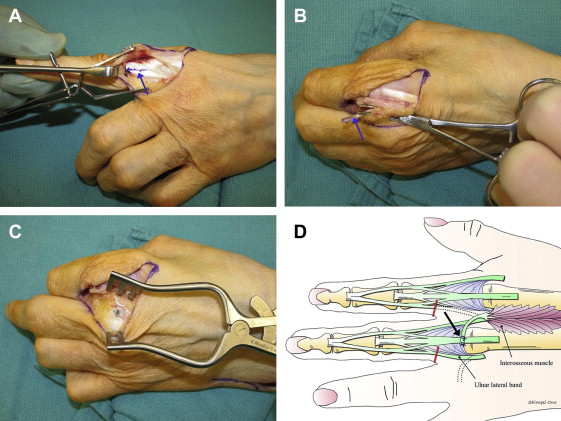
If the MCPJ is not too involved and the fingers are drifted ulnarly but can be reduced to the natural posture easily, a crossed intrinsic transfer procedure is preferred ( Fig. 5 ). Past studies have shown that the procedure can provide an effective long-term correction for ulnar drift. Crossed intrinsic transfers are performed in conjunction with MCPJ synovectomy and soft tissue reconstruction (centering of extrinsic extensor tendons and repair or reefing of radial collateral ligaments and joint capsules). The ulnar lateral bands of the index, long, and ring fingers are transferred to the long, ring, and small finger extensor tendons or the radial lateral band in an effort to add more radial pull to the fingers. Rather than releasing the ulnar intrinsic tendons, the tendons may be used to reinforce the radial supporting structures of the adjacent fingers. The radial sagittal band of the affected finger is tightened to centralize its extensor tendon, because no ulnar intrinsic tendon is available for transfer.
MCPJ arthroplasty
Severe deformities at the MCPJ may manifest as joint destruction, chronic subluxation, and severe ulnar deviation. The ligamentous contractures around the joints cannot be corrected by soft tissue reconstruction alone. In most cases, silicone implants are the most reliable arthroplasty technique to replace destroyed joints. A recent prospective study showed significant improvement for patients with RA with poor baseline function treated with the silicone metacarpophalangeal arthroplasty (SMPA) compared with the nonsurgical group. Significant pain unresponsive to conservative treatments and impaired function were strongly associated with patients who chose surgical treatment. MCPJ arthroplasty must be limited to patients with severe functional impairments because some patients with major deformities can maintain a reasonable level of function, which may not improve significantly after joint reconstruction. MCPJ arthroplasty also has the advantage of shortening the bone at the MCPJ, decreasing the tension on the tendons and ligaments contributing to the ulnar deformity. Although various procedures are available for joint replacements, SMPA is the most widely used and studied for the MCPJ. Silicone implants are easy to place, can be revised without much difficulty, and are reasonable in cost. These implants differ in fixation, articulation, and motion from other joint replacement prostheses. The silicone prosthesis acts as a spacer between the metacarpal and proximal phalanx. The pistoning or gliding of the implant within the medullary canal is thought to add to the range of motion achieved by the arthroplasty and to disperse the forces along the implant–bone interface. If an SMPA is performed, one of the most important considerations is the restoration of function. The literature indicates that one can anticipate an arc of motion within the 50° range, with improvement of extensor lag. Improvement of ulnar deviation also occurs, although some ulnar drift tends to recur over time. Recent studies have shown that outcomes for the ulnar digits seem to be worse than those for the radial digits after SMPA. Although the radial fingers can be aligned readily, achieving a satisfactory reduction for the ring and particularly the small finger may be difficult. To achieve sufficient correction of the deformities in the ulnar fingers, adequate bone resection and careful realignment of the extensor mechanism are essential, and the abductor digiti minimi tendon is sometimes divided to release the small finger. Another important outcome after MCPJ arthroplasty is the improvement in the appearance of the hand. The use of silicone implants have been shown to effectively correct ulnar drift deformities and improve the appearance of the rheumatoid hand. Short-term functional and aesthetic outcomes of the SMPA procedures are impressive, but long-term studies have shown a high rate of breakage from imperfections of silicone used as an arthroplasty material. Silicone implant fracture rates average at 2% of cases (range, 0%–38%). Fortunately in most cases, implant fractures do not require revision of the prosthetic component; many authors report that most patients with fractured implants retain an acceptable level of function and do not require further surgery.
PIPJ
The two main deformities at the PIPJ are the swan-neck deformity and the boutonniere deformity.
Swan-neck deformity
Swan-neck deformity is characterized by hyperextension of the PIPJ with reciprocal flexion of the MCPJ and distal interphalangeal joint (DIPJ) ( Fig. 6 ). A swan-neck deformity can occur from a disorder at the wrist, MCPJ, PIPJ, or DIPJ. The pathogenesis of wrist and MCPJ deformity was described earlier. At the PIPJ, the synovial pannus distends the joint and stretches the dorsal surface of the volar plate. This synovitis leads to stretching, weakening, and eventually destruction of the volar plate and collateral ligaments, and the insertion of the flexor digitorum superficialis (FDS), resulting in loss of palmar restraint at the PIPJ. This effect allows the normal extensor forces to cause abnormal hyperextension of the PIPJ that in turn relaxes the normal tension on the conjoint lateral bands, leading to dorsal migration. A relaxed conjoint lateral band loses the ability to extend the DIPJ. In addition, the hyperextension of the PIPJ stretches the flexor digitorum profundus (FDP) through increasing its flexor action of the DIPJ and causes the loss of the mechanical advantage of the oblique retinacular ligament in extending the DIPJ. This loss of conjoint lateral band and oblique retinacular ligament tension and increased tension of the FDP results in a DIPJ flexion deformity. Over time, adhesions develop between the central slip and the dorsally translated conjoint lateral bands, converting the flexible deformity to a fixed deformity. DIPJ synovitis can cause weakening and rupture of the terminal extensor tendon insertion, leading to the development of a mallet deformity. The proximal migration of the terminal extensor insertion will cause the lateral bands to become lax. All the power of the common extrinsic extensor will now be directed toward the central slip that inserts into the middle phalanx. Over time, the volar supporting structures of the PIPJ are weakened and the PIPJ is forced into hyperextension, resulting in a swan-neck deformity.
Related posts:
 Free Functional Muscle Transfer for the Upper Extremity
Free Functional Muscle Transfer for the Upper Extremity
 Scar Contractures of the Hand
Scar Contractures of the Hand
 Functional Reconstruction of the Hand: The Stiff Joint
Functional Reconstruction of the Hand: The Stiff Joint
 Current Status of Brachial Plexus Reconstruction: Restoration of Hand Function
Current Status of Brachial Plexus Reconstruction: Restoration of Hand Function
 Treatment of Nonunion and Malunion Following Hand Fractures
Treatment of Nonunion and Malunion Following Hand Fractures
 Thumb Reconstruction
Thumb Reconstruction
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


