Ischemia of the hand remains an uncommon condition, but problems with arterial perfusion of the hand can arise from trauma (open and closed), thrombosis, or arteriovascular disease. Certain identifiable patterns are seen with hand ischemia, usually discernable according to which one of the major arteries (radial or ulnar) are involved. This article discusses the origin and management of ischemic hand conditions, with an emphasis on recognizing the patterns of ischemia that are commonly seen.
Ischemia of the hand remains an uncommon condition, but problems with arterial perfusion of the hand can arise from trauma (open and closed), thrombosis, or as a result of arteriovascular disease. Certain identifiable patterns are seen with hand ischemia, usually discernable according to which one of the major arteries (radial or ulnar) are involved. This article discusses the origin and management of ischemic hand conditions, with an emphasis on recognizing the patterns of ischemia that are commonly seen.
Arterial anatomy of the hand
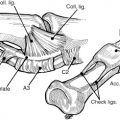
The vascularity of the hand is primarily provided by the radial and ulnar arteries, with secondary contribution through the anterior and posterior interosseous vessels that arborize at the wrist. Although these interosseous vessels do not supply the dominant blood supply to the hand, they may become important in some ischemic conditions involving the major two vessels. The arterial anatomy in the palm has traditionally been considered as having a deep and a superficial arch, whose names describe their positions in the palm. The deep arch is typically fed by the radial artery as it comes around the hand at the base of the thumb in the anatomic snuff-box, and then enters the palm as it pierces the dorsal interosseous muscle in the first web space. This artery then connects with the deep component of the palmar arch. The ulnar artery runs into the palm from the forearm along the radial aspect of the pisiform bone with the ulnar nerve on its ulnar side. This artery continues on to become the superficial arch and supplies the proper digital vessels in the palm. Since the early work of Coleman and Anson on the anatomy of the arch, much discussion has surrounded the potential for ischemia from an incomplete arch if one of the major vessels of the hand becomes occluded. Traditional teaching is that most hand ischemia is caused by this incomplete arch, and the fingers become ischemic from lack of crossover blood flow from the nonthrombosed vessel. In the authors’ experience with close to 150 cases of arterial thrombosis of the radial or ulnar arteries, ischemia of the fingers or hand is not generally from a lack of connection between the two portions of the arch, but rather from embolization of clots from the site of original thrombosis (in the radial or ulnar artery) into the downstream digital vessels, leading to ischemia of the fingers fed by these digital arteries ( Fig. 1 ). Thus, the authors question the long-held concern about the lack of a complete palmar arch in its contribution to digital ischemia with thrombosis of the radial or ulnar arteries. Some patients unquestionably have an incomplete arch and would experience partial hand ischemia if the radial or ulnar arteries were harvested for a bypass or flap, but in the authors’ experience, these patients are significantly few and far between.

Numerous causes of ischemia of the upper extremity have been reported ( Box 1 ). The treatment should be individualized depending on the cause and expected outcomes.
Occlusive arterial disease
Atherosclerosis
Embolic disorders
Vasculitis
Thromboangiitis obliterans
Thoracic outlet syndrome
Takayasu disease
Traumatic aneurysm
Canalization
Ulnar hammer
Arteriovenous steal/shunt
Arteriovenous malformation
Vasospastic disorders
Cutaneous small-vessel disease
Vasculitis
Waldenström’s hypergammaglobulinemic purpura
Henoch-Schönlein purpura
Collagen vascular–associated
Acute hemorrhagic edema of infancy
Rheumatoid nodules with vasculitis
Urticarial vasculitis
Hyperimmunoglobulinemia D syndrome
Essential mixed cryoglobulinemia
Familiar Mediterranean fever
Connective tissue disorders
Myeloproliferative disorders
Iatrogenic hand ischemia
Accidental blunt or sharp injury to the radial, ulnar, palmer, or digital vessels may result in vascular insufficiency to the hand or digits. The vascular system could also be disrupted from surgical intervention through flap harvesting. Ischemia from harvesting of the radial artery for coronary artery bypass grafting or flap transfer is fortunately uncommon. Although cases of digital ischemia have been reported after this, most studies have shown no significant morbidity from harvest of the radial artery, either for coronary bypass or transfer of a radial forearm flap. Several studies in patients undergoing coronary artery bypass with the radial artery have actually shown improved perfusion of the radial digits after harvest, presumably because of a compensatory mechanism to increase flow to the fingers supplied primarily by the radial artery. Although ischemia of the digits after radial artery harvest has an estimated incidence of 10%, some investigators have found no clinical evidence (hand claudication or ischemic symptoms) after harvest. If the hand is noted to be ischemic after harvest of the radial artery for either a flap or coronary bypass, performing a vein bypass graft at that time is probably prudent rather than waiting for symptoms to develop.
Another potential iatrogenic cause of hand ischemia is radial artery catheterization for blood pressure monitoring. Large studies have shown the overall safety of radial artery catheterization, with one study quoting a “permanent ischemic complications” rate of only 0.09%. Nonetheless, other large studies have shown flow abnormalities or thrombosis of the radial artery in approximately 26% of patients who have an arterial line. Ischemia significant enough to lead to digital amputation is rare but is certainly reported. In their review of eight patients who experienced ischemia of the fingers after radial artery catheterization, Valentine and colleagues found that all surviving patients developed some gangrene in the hand and most required some level of digital amputation. This article’s authors have had three patients in the past 20 years who required significant amputations after radial artery cannulation: one of the entire hand and two of partial hands. All three of these patients had been taking intravenous vasopressor agents for hypotension, which probably worsened the ischemia of the hand after thrombosis of the radial artery.
Geschwind and colleagues believed that their experience did not support surgical intervention, because their patients all subsequently experienced ongoing ischemic problems. They believed that this was because of embolization of a clot to the digits that could not be removed. Although managing these patients with thrombolytic agents might be theoretically beneficial, this article’s authors’ experience has been that radiologists consider this treatment to present too much of a systemic risk for most of these patients. Therefore, the authors believe that these patients should be explored and have thrombectomy of the radial artery and repair of the damaged segment of artery performed whenever possible. Even if this is unsuccessful, the authors consider the risk to be justified if amputation of a significant portion of the hand can be prevented ( Fig. 2 ).
Iatrogenic hand ischemia
Accidental blunt or sharp injury to the radial, ulnar, palmer, or digital vessels may result in vascular insufficiency to the hand or digits. The vascular system could also be disrupted from surgical intervention through flap harvesting. Ischemia from harvesting of the radial artery for coronary artery bypass grafting or flap transfer is fortunately uncommon. Although cases of digital ischemia have been reported after this, most studies have shown no significant morbidity from harvest of the radial artery, either for coronary bypass or transfer of a radial forearm flap. Several studies in patients undergoing coronary artery bypass with the radial artery have actually shown improved perfusion of the radial digits after harvest, presumably because of a compensatory mechanism to increase flow to the fingers supplied primarily by the radial artery. Although ischemia of the digits after radial artery harvest has an estimated incidence of 10%, some investigators have found no clinical evidence (hand claudication or ischemic symptoms) after harvest. If the hand is noted to be ischemic after harvest of the radial artery for either a flap or coronary bypass, performing a vein bypass graft at that time is probably prudent rather than waiting for symptoms to develop.
Another potential iatrogenic cause of hand ischemia is radial artery catheterization for blood pressure monitoring. Large studies have shown the overall safety of radial artery catheterization, with one study quoting a “permanent ischemic complications” rate of only 0.09%. Nonetheless, other large studies have shown flow abnormalities or thrombosis of the radial artery in approximately 26% of patients who have an arterial line. Ischemia significant enough to lead to digital amputation is rare but is certainly reported. In their review of eight patients who experienced ischemia of the fingers after radial artery catheterization, Valentine and colleagues found that all surviving patients developed some gangrene in the hand and most required some level of digital amputation. This article’s authors have had three patients in the past 20 years who required significant amputations after radial artery cannulation: one of the entire hand and two of partial hands. All three of these patients had been taking intravenous vasopressor agents for hypotension, which probably worsened the ischemia of the hand after thrombosis of the radial artery.
Geschwind and colleagues believed that their experience did not support surgical intervention, because their patients all subsequently experienced ongoing ischemic problems. They believed that this was because of embolization of a clot to the digits that could not be removed. Although managing these patients with thrombolytic agents might be theoretically beneficial, this article’s authors’ experience has been that radiologists consider this treatment to present too much of a systemic risk for most of these patients. Therefore, the authors believe that these patients should be explored and have thrombectomy of the radial artery and repair of the damaged segment of artery performed whenever possible. Even if this is unsuccessful, the authors consider the risk to be justified if amputation of a significant portion of the hand can be prevented ( Fig. 2 ).
Closed vascular trauma
Ulnar Artery Thrombosis
The most common cause of ischemia of the hand is closed trauma to the vessels of the hand, primarily the ulnar artery. This condition is usually caused by banging of the ulnar side of the hand, often repetitively, and has been dubbed the hypothenar hammer syndrome . It is the result of trauma to the ulnar artery in Guyon’s Canal, leading to thrombosis and symptoms of ischemia of the digits. The vascular insufficiency is often found in the ring and little finger and is commonly associated with numbness and tingling in the ulnar nerve–innervated digits. The ulnar nerve may be contused during injury to the ulnar artery, or can simply become involved through its proximity to the inflamed and thrombosed ulnar artery. The thrombosed ulnar artery often becomes tortuous and aneurysmal. Physical examination of these patients will show ischemic digits (and perhaps gangrene or ulceration), and the ulnar artery at the wrist will often still be palpable. An Allen test will usually confirm occlusion of the ulnar artery, but the authors prefer to perform what they call a “dynamic Doppler examination” through listening to the arch with a pencil Doppler and then sequentially occluding the ulnar and radial arteries at the wrist with digital pressure. This technique provides a much better idea of which vessel may be thrombosed. They also prefer to listen to the digital pulps with the pencil Doppler to confirm which fingers have experienced occlusion of the digital arteries from embolization of clot. Patients who have experienced embolization of clot to the digital vessels will usually have recanalization of these vessels after excision and bypass of the injured ulnar artery, and will thus have return of their Doppler pulp signals at some point after bypass.
The natural history of untreated hypothenar hammer syndrome has been somewhat difficult to ascertain. Most surgeons believe that symptomatic patients should probably be managed surgically. A recent study from France, however, analyzed 47 patients who presented to the Department of Internal Medicine at the University of Rouen with hypothenar hammer syndrome (which represented 1.13% of all patients referred for symptoms of Raynaud’s disease). They noted that 92% of these patients had “occupational exposure to repetitive palmar trauma.” Arteriography showed thrombosis of the ulnar artery in the palm (60%) or ulnar artery aneurysm (40%); 57% were noted to have “embolic multiple occlusions of the digital arteries.” Only two of these patients were managed surgically, and these individuals had nonthrombotic ulnar artery aneurysms and continued to be symptomatic on conservative management (probably from recurrent embolization, in the authors’ opinion). The remainder of the patients were managed with a variety of conservative measures. All were counseled to change occupational exposure. All received vasodilators (calcium channel blockers and buflomedil), others also received platelet aggregation inhibitors, and some received hemodilution therapy (intravenous dextran) to lower the hematocrit to 35%. Three patients required a 5-day course of intravenous prostacyclin infusion to manage digital necrosis. Ulcers took an average of 1.6 months to heal on this varied regimen, and, significantly, 28% of patients treated conservatively exhibited recurrent symptoms at an average of 11 months after the initial episode. Among these patients, two had undergone thoracic sympathectomy, but none had undergone surgical bypass of the lesion in the ulnar artery. This study is certainly the only large one examining patients with traumatic ulnar artery thrombosis managed conservatively, and although the results may look encouraging, these patients were managed very aggressively from the nonsurgical standpoint. Approximately 50% of patients required a several-day hospitalization for administration of intravenous dextran or prostacyclin. Each of these drugs has its own inherent potential side effects. With a recurrence rate near 30% in patients treated nonsurgically, the authors believe that bypass should be strongly considered in patients who remain symptomatic on straightforward management with calcium channel blockers and aspirin. This approach seems to be supported by the literature.
In a follow-up of 14 patients with hypothenar hammer syndrome, Zimmerman and colleagues performed digital blood pressure measurements on each patient to calculate the digital brachial index, which is the digital blood pressure divided by the ipsilateral arm brachial artery blood pressure. Patients with a value greater than 0.7 were managed with simple ligation of the artery and excision, whereas those with a value less than 0.7 were managed with excision and bypass. Through excising the ulnar artery, a Leriche’s sympathectomy was being performed in the patients who did not have severe diminution of flow. All patients experienced improvement after bypass, but no statistical difference was seen in long-term results between these groups. However, the investigators did not manage any patients without surgery.
More recently, Lifchez and Higgins reported similar findings in an evaluation of 14 patients who underwent surgery for ulnar artery thrombosis. Two patients had primary excision of the involved segment and direct repair, and the other 12 had the ulnar artery reconstructed with a reversed vein graft. Eight of 12 grafts (67%) were patent at an average of 52 months’ follow-up. All patients experienced improvement in their digital brachial index and subjective symptoms, with those who had experienced thrombosis showing the best improvement in the digital brachial index. Based on the results, the investigators suggest performing reconstruction on patients in whom medical management fails to relieve symptoms, those whose digital soft tissue ulcers fail to heal with conservative management, and those with a reconstructible lesion. Koman’s group found similar results in their review of 13 hands in 12 patients with ulnar artery thrombosis. None of the patients had collagen vascular disease, and they found a 77% patency rate of bypass grafts at 24 months’ follow-up. Of the three patients who had thrombosis of their grafts, two were symptomatic and one was not. The investigators concluded that patients with posttraumatic ulnar artery thrombosis managed with bypass grafting had decreased symptoms and improved function, and experienced a positive effect on health-related quality of life, which confirmed the findings of an earlier study by this group.
Based on these studies and the authors’ personal experience, the authors believe that most patients who experience thrombosis of the ulnar artery from external trauma will benefit from either excision and repair of the damaged segment or vein graft bypass. The authors usually manage patients conservatively for a short period with aspirin and calcium channel blockers but, if the patients have or develop gangrene or ulcerations, or the ischemic symptoms do not improve, will proceed with surgical management. With the current widespread training in microvascular surgical techniques and the ease of performing a vein graft, the authors also believe that bypass, rather than simple excision, should be performed in almost all patients. The morbidity of harvesting a vein graft is minimal, and the studies described earlier confirm that increasing inflow will improve symptoms.
In a review of roughly 100 patients who had experienced thrombosis of the ulnar artery, the authors found that 44% presented with ischemic symptoms in the ring finger, whereas 33% had ischemia of the middle finger, 24% had ischemia of the little finger, and 23% had ischemia of the index, but only 2% of patients had evidence of thumb ischemia (most patients had ischemia of more than one finger, thus the results tally more than 100%). Thus, the pattern of digital ischemia seen with ulnar artery thrombosis rarely involves the thumb. The primary cause of ischemia in these individuals is embolization of clot from the original site of injury to the common and proper digital arteries, which leads to the digital ischemia of the involved fingers. The pattern of thrombosis in patients with hypothenar hammer syndrome is typical, because the vessel will usually clot from and to where adequate outflow is present. This process leads to the vessel thrombosing distally to the point at which the superficial arch comes across and anastomoses with the common digital vessel to the fourth web space, and proximally back to either the deep branch in the palm (accompanying the deep motor branch of the ulnar nerve) or, more commonly, the level of the dorsal branch of the ulnar artery (which usually accompanies the dorsal sensory branch of the ulnar nerve). This pattern is commonly seen on arteriograms of the hands in patients with hypothenar hammer syndrome ( Fig. 3 ). Patients in a hypercoagulable state or those with collagen vascular disease who experience thrombosis of the ulnar artery may have more extensive occlusion, depending on the severity of their disease.
Related posts:
 Free Functional Muscle Transfer for the Upper Extremity
Free Functional Muscle Transfer for the Upper Extremity
 Scar Contractures of the Hand
Scar Contractures of the Hand
 Functional Reconstruction of the Hand: The Stiff Joint
Functional Reconstruction of the Hand: The Stiff Joint
 Current Status of Brachial Plexus Reconstruction: Restoration of Hand Function
Current Status of Brachial Plexus Reconstruction: Restoration of Hand Function
 Treatment of Nonunion and Malunion Following Hand Fractures
Treatment of Nonunion and Malunion Following Hand Fractures
 Thumb Reconstruction
Thumb Reconstruction
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


