Reconstruction of the Ear Lobe
Matthew M. Hanasono
DEFINITION
Ear lobe defects can result following trauma or following resection of cutaneous malignancies.
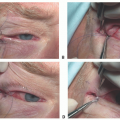
The simplest types of resection and reconstruction for skin cancers on the ear lobe are amputation-type resections. These can be carried out along a curved line to approximate the curvature of the lower border of the ear lobe. Most of the procedures will result in loss of volume or height (ptosis) of the lobule.
The ear lobe is difficult to reproduce surgically because it has a characteristic protuberance that consists of fibrofatty tissue rather than cartilage.
Most require more than a one-stage operation.
ANATOMY
Ear lobes (ear lobules) occur in the lower third of the ear. They consist of areolar and fibrofatty tissue and lack cartilage.
The ear lobes are usually about 2 cm long and may or may not be attached to the cheek to a variable degree, a characteristic that is thought to be inherited.
The ear lobe should lie roughly even at the level of the nasal ala, which is typically half the distance between the eyes and mentum.
PATIENT HISTORY AND PHYSICAL FINDINGS
A thorough history and physical should be obtained prior to any operation paying close attention to significant comorbidities, including smoking history, and prior surgeries including scars in the area that may impact the design preauricular and postauricular flaps.
Preauricular and postauricular skin laxity should be assessed to plan whether a single folded flap can be used or if doubleopposing flaps will be required.
For example, young patients and patients who have had a face-lift may not have adequate preauricular skin laxity to create a flap and still close the donor site primarily. Sentinel lymph node biopsy and neck dissection incisions may also preclude some local flaps.
IMAGING
Patients who have undergone resection for cutaneous malignancies such as melanoma and squamous cell carcinoma may require imaging studies for staging and to rule out potential for metastatic disease.
SURGICAL MANAGEMENT
Numerous reconstructive techniques have been described to restore the ear lobe, all based on single or double local flaps.
Based on the availability of preauricular and postauricular tissue, a single folded flap or double-opposing flaps can be used for ear lobe reconstruction.
Single flaps are usually folded and may be designed as bilobed flaps.
Use of an anteriorly based transverse folded flap is known as Gavello procedure.3
The advantage of this procedure is that it is usually a single-staged procedure. A cartilage graft may be added to give support and prevent contracture, and the donor site is usually skin grafted.
The negative is the long length of the flap and the possibility of a donor-site scar (FIG 1A).
Folded preauricular or postauricular flaps usually need a thin cartilage graft to maintain ear lobe height (FIG 1B).
Double-flap reconstruction with preauricular and postauricular skin flaps usually does not require grafts (FIG 1C,D).6Related posts:
 Mandible Reconstruction With Fibula Flap With Templates
Mandible Reconstruction With Fibula Flap With Templates
 Lower Lip Reconstruction With the Nasolabial Flap
Lower Lip Reconstruction With the Nasolabial Flap
 Lateral Tarsal Strip Canthoplasty
Lateral Tarsal Strip Canthoplasty
 Antia-Buch Flaps for Ear Reconstruction
Antia-Buch Flaps for Ear Reconstruction
 Pectoralis Major Flap for Pharyngeal Reconstruction
Pectoralis Major Flap for Pharyngeal Reconstruction
 Facial Reanimation in the Oncologic Patient Using Nerve Grafts and Nerve Transfers
Facial Reanimation in the Oncologic Patient Using Nerve Grafts and Nerve Transfers

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


