(1)
Yotsuya Medical Cube, Chiyoda-ku, Tokyo, Japan
Selectable Flaps for Mediastinitis / Pyothorax
Pectoralis major muscle flap
Rectus abdominis muscle flap
Latissimus dorsi musculocutaneous flap
Selectable Methods for Abdominal Hernia Reconstruction
The difficulty level of each surgical procedure is shown subsequent to the procedure title (e.g., Level of Difficulty: 2). The levels range from 1 to 5, with level 1 indicating a preliminary level and level 5 indicating a very advanced level.
11.1 Mediastinitis: Pectoralis Major Muscle Flap (Level of Difficulty: 2)
Information
Vascular pedicle Thoraco-acrominal artery, Lateral thoracic artery
Indication In cases where the range of osteomyelitis of the sternum is narrow, and amount of defect bone in the center of the sternum following debridement is comparatively superficial.
11.1.1 Operation Procedures

Fig. 11.1
Procedure 1: Subcutaneous fistula that developed after heart surgery. Small amount of gentian violet is injected into the fistula to dye the fistula area

Fig. 11.2
Procedure 2: The stained area is then completely debrided. If the necrotic section of the fistula and sternum is small, and the tissue vessels are not large, then a pectoralis major muscle transfer is indicated
Note
If there is a large tissue defect, then a latissimus dorsi musculocutaneous flap is indicated, and if the defect is deep, then a rectus abdominis muscle flap transfer is indicated.
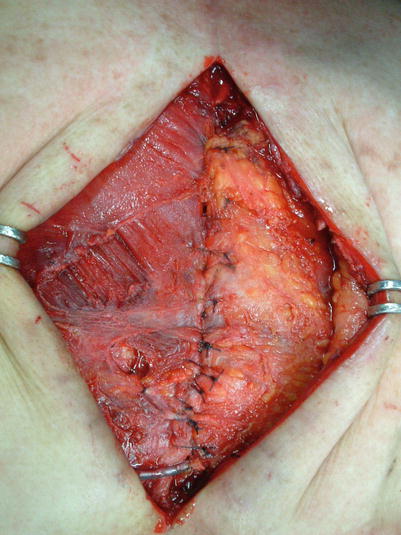

Fig. 11.3
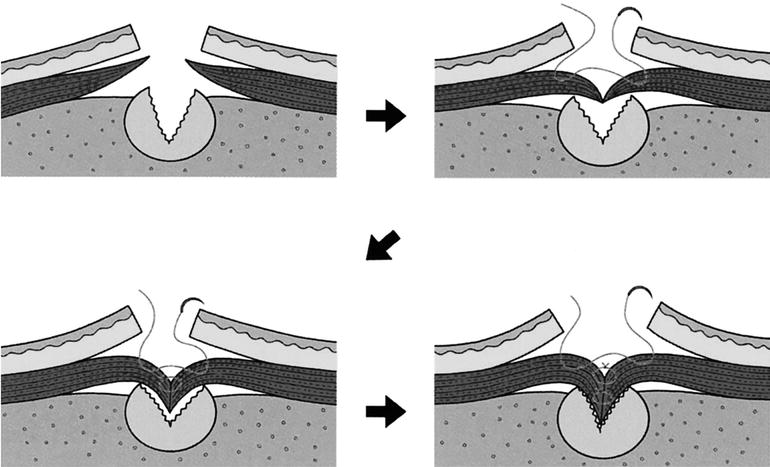
Procedure 3: The section of pectoralis major muscle attached to the sternum is carefully and broadly detached and the full length of the muscle margin of pectoralis major is completely removed. A mattress suture is performed to both sides to incorporate the flap into the tissue defect area. By repeating uniformly for the whole length and conducting several layers of suturing, the flap gradually fills the tissue defect area
Fig. 11.4
Procedure 4: A continuous suction drain is inserted subcutaneously above the flap, and the wound closed
Tips
Make sure to conduct sufficient debridement of the infectious wound
Dyeing by injecting gentian violet into the fistula is essential to make sure sufficient debridement is conducted of infectious wounds.

11.2 Mediastinitis: Rectus Abdominis Musculocutaneous Flap (Level of Difficulty: 4)
Information
Vascular pedicle Right superior epigastric artery and internal thoracic artery
Size Full length of rectus abdominis muscle
Indication For filling the lost tissue following debridement of infectious sternum in lower part of chest.
Disadvantage Often insufficient amount of tissue to cover/fill upper chest in vicinity of sternoclavicular joint. In such cases a pectoralis major muscle flap or latissimus dorsi muscle flap transfer is also carried out.
Caution In many cases involving heart surgery, the left internal thoracic artery has already been used, so elevate the right internal thoracic artery for use as the muscle flap pedicle.
11.2.1 Operation Procedures

Fig. 11.5
Procedure 1: A subcutaneous fistula was recognized in the vicinity of the hypochondrium following heart surgery

Fig. 11.6
Procedure 2: Gentian violet is injected from the fistula to dye the area, and the fistula is completely debrided
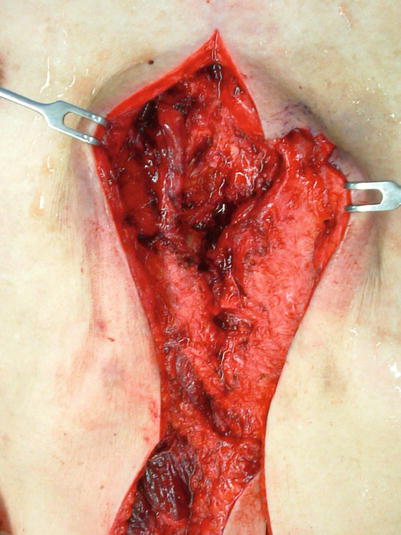
Fig. 11.7
Procedure 3: Although the range of the fistula is narrow, it is deep, so filling using a rectus abdominis muscle flap is planned, and a longitudinal incision extended to the abdominal region
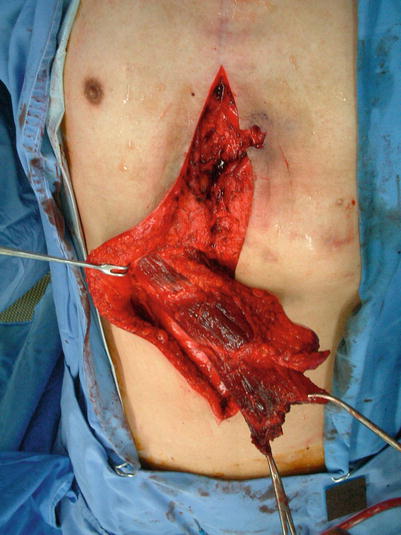
Fig. 11.8
Procedure 4: The left internal thoracic artery had already been used in heart surgery so the rectus abdominis muscle flap with monitoring skin was raised from the right side. The rectus abdominis muscle is severed toward the periphery with sufficient length in consideration of the overlap margin, and the deep inferior epigastric blood vessels running along the rear of the flap ligated and cut. The flap is rotated to the proximal side
Note
If the skin flap is not attached, the muscle flap is turned over to the proximal side.

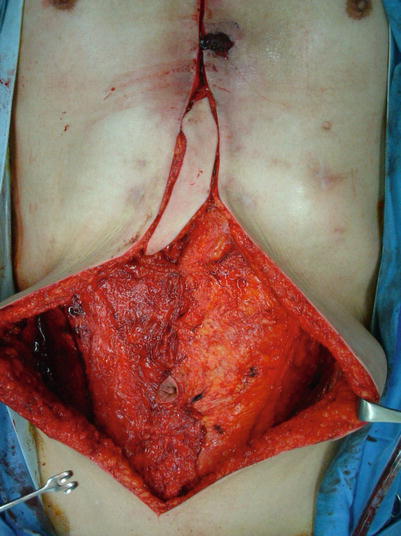
Fig. 11.9
Procedure 5: The tissue defect area beneath the fistula is filled using the muscle flap section, and the surrounding area sutured in place
Fig. 11.10
Procedure 6: The entire length of the bilateral external oblique muscle is cut longitudinally in accordance with the components separation method, and the medial margin of the affected external oblique muscle sutured to the unaffected contralateral rectus abdominis muscle, and the donor site closed
Refer to Section of
“Reconstruction of mediastinitis, pyothorax, abdominal incisional hernia/Abdominal incisional hernia: Components Separation Method” in Chap.11
Please also see the Tips “Apply the Components Separation Method to close up the donor site”.

Fig. 11.11




Procedure 7: A continuous suction drain is inserted subcutaneously in the chest/abdomen region, and the wound closed
Related posts:





Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
