Reconstruction of Buccal Mucosal Defects
Imran Ratanshi
Colleen McCarthy
DEFINITION
Carcinoma can involve the buccal mucosa of the oral cavity.
The treatment of buccal mucosa cancer is typically surgical resection.
ANATOMY
The buccal mucosa lines the inner aspect of the cheek and the lip.
Blood supply to the buccal mucosa is derived from buccal branches of the facial artery, superficial temporal artery, and internal maxillary artery.
Sensory innervation to the buccal mucosa is provided by the trigeminal nerve.
Anatomic borders (FIG 1A)
Superiorly border—attachments to the maxillary alveoli
Inferior border—attachments to the mandibular alveoli
Anterior border—lateral lip commissure
Posterior border—pterygomandibular raphe
Relevant layers of the cheek from external to internal (FIG 1B)
Skin
Subcutaneous fat
Superficial musculoaponeurotic system (SMAS)/platysma
Parotid fascia/capsule
Parotid gland
Parotidomasseteric fascia
Masseter muscle
Buccal fat pad (within buccal space)
Buccinator
Buccal mucosa
There are three important spaces in the buccal region. These are potential sites for fluid collection, infection, or tumor spread.
Buccal space
Anterior border—oral commissure
Posterior border—anterior border of masseter
Superior border—zygomatic process of maxilla, zygomaticus muscles
Inferior border—depressor anguli oris and attachment of deep fascia to mandible
Medial border—buccinator muscle (space is superficial to the muscle)
Lateral border—platysma, subcutaneous tissue, skin
Pterygomandibular space
Anterior border—posterior border of buccal space (anterior border of masseter)
Posterior border—parotid gland
Superior border—lateral pterygoid muscle
Inferior border—inferior border of mandible (lingual surface)
Lateral border—ascending ramus of mandible (space is deep to mandible)
Medial border—medial pterygoid muscle (space is superficial to this muscle)
Masseteric (or submasseteric) space
Anterior border—anterior margin of masseter
Posterior border—parotid gland
Superior border—zygomatic arch
Inferior border—mandible
Lateral border—masseter
Medial border—lateral surface of mandibular ramus
The buccal fat pad (of Bichat) occupies the buccal space. Contents of the buccal fat pad include
Motor buccal nerve
Sensory buccal nerve (V3)
Facial artery and vein
Buccal branch of maxillary artery
Terminal buccal branches of facial nerve
Parotid (Stensen) duct
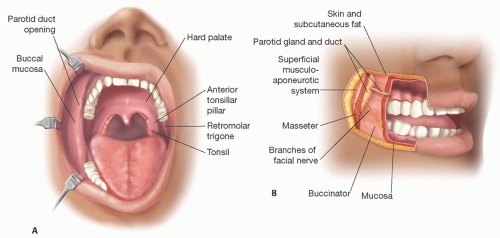 FIG 1 • A. Surface anatomy of the intraoral cheek surface. B. Anatomic layers of the cheek illustrated from external to internal. SMAS, superficial musculoaponeurotic system. |
PATHOGENESIS
Buccal cancer originates in the mucosal lining of the cheeks inside the mouth.
Squamous cell carcinoma is the most common type of pathology.
No single risk factor causes buccal cancer.
Risk factors for buccal cancer include a history of:
Premalignant conditions1
Oral lichen planus and leukoplakia are common premalignant lesions.
Malignant conditions
Previous aerodigestive cancer
Tobacco (particularly chewing tobacco)
Alcohol abuse
Betel nut [or areca nut] (common in a South Asian chewed delicacy called “paan”)
Poor nutrition
Poor dentition
Oral denture wear
Viruses: HPV-16, HPV-18, HPV-31, HPV-33, and HPV-35; HHV-4 and HHV-8; HIV; EBV1
PATIENT HISTORY AND PHYSICAL FINDINGS
Risk factors for buccal cancer should be identified, particularly smoking status. In a patient who is an active smoker, the risk of partial or complete flap loss is greater.
A history of any prior surgeries or vascular line placement may limit the use of specific reconstructive options.
For example, a prior neck dissection may preclude the use of the facial artery musculomucosal (FAMM) flap if the facial artery has been previously ligated.
If level 1 (submental) nodes have been previously resected, use of the submental island flap or platysmal island flap is contraindicated.
Placement of a radial artery line for invasive blood pressure monitoring is a relative contraindication for use of a radial forearm free flap.
History and clinical findings of prior irradiation may also be a relative contraindication to a locoregional flap reconstruction, depending on the condition of the tissues.
A handheld pencil Doppler or duplex ultrasound can be used in the preoperative setting and/or in the operating room to determine the location of arterial perforating vessels.
SURGICAL MANAGEMENT
Preoperative Planning
Potential donor sites must be considered preoperatively.
Discussion with the resecting surgeon is helpful to estimate the defect size and potential for close or positive margins. If positive margins are anticipated, other nonsurgical treatment strategies should be explored.
Need for adjuvant radiation therapy should influence the reconstructive modality.
It is imperative that patency of the ulnar artery is confirmed with an Allen test in the preoperative period. Use of a bedside pulse oximeter can be a useful adjunct to objectively identify collateral flow in this setting.
Intravenous and intra-arterial lines must also be avoided in the ipsilateral upper forearm if a radial forearm free flap is to be harvested.
Positioning
The patient is placed in a supine position with neck in slight extension.
General anesthesia with nasotracheal intubation will typically be employed.
Tumor ablation will proceed by the ablative surgeon.
The reconstructive surgeon may undertake simultaneous harvest of a microvascular flap if the surgical teams are certain that a free tissue transfer is indicated. Partial elevation of a flap may be employed, including pedicle dissection, and may be performed to optimize efficiency.
Approach
The pliable nature of buccal mucosa allows for full mandible excursion. Therefore, primary closure of small to moderatesized defects can lead to soft tissue restriction, ultimately resulting in trismus.
Superficial mucosa-only defects can be reconstructed with a split-thickness skin graft or palatal graft.
Alternatively, acellular dermis may be used in this setting and can serve as a scaffolding in which vascular ingrowth can occur with minimal scar contraction.
Flap reconstruction may be indicated in circumstances where more bulk is desired than can be achieved with skin or dermal grafting alone.
Many local and locoregional flap options have been described. Workhorse flaps utilized in restoring buccal mucosal lining include
Pedicled flap options:
Buccal fat transposition flap—for small buccal defects
Facial artery myomucosal flap—small to moderatesized buccal defects that involve the alveoli and/or lips
Submental artery island flap—moderate-sized buccal defects
Platysmal island flap—moderate-sized buccal defects
Pectoralis major flap—moderate- to large-sized buccal defects in patients who are poor candidates for free flap reconstruction or in salvage cases
Microvascular free flap options—offer additional tissue bulk and the ability to contour donor tissue to fit a defect without restriction
Radial forearm fasciocutaneous flap
Thin, pliable soft tissue
Consistent blood supply with long vascular pedicle
Donor-site morbidity includes tendon exposure, injury to the dorsal radial sensory nerve branch, and inferior appearance.
Anterolateral thigh fasciocutaneous flap
Can often close donor site primarily
Best used in very thin patients or those in whom a radial forearm flap is not an option
Can be performed as adipofascial flap if more bulky donor site
TECHNIQUES
▪ Autogenous Grafts
For mucosa-only defects, very small defects may be repaired with primary closure. Small defects may be repaired with palatal mucosal grafts. For moderate-sized defects, a split-thickness skin graft can be employed to resurface the intraoral buccal lining.
Skin grafts should be fenestrated to prevent accumulation of serous fluid and fixed with resorbable suture (eg, cat gut).3
A tie-over bolster dressing using petroleum-impregnated gauze and nonresorbable suture (eg, silk) should be used to minimize shear and prevent saliva from entering below the skin graft surface.4 The bolster can also be tied extraorally.3
A bite block may be considered if there is concern about dislodging the bolster dressing.
Grafts should not be considered in the setting of anticipated radiation.
▪ Acellular Dermal Matrix
Human acellular dermal matrix (ADM) is a biomaterial derived from cadaveric skin that has been processed to remove cells and immunogenic antigens.
ADM may be used in a similar manner to a skin graft.
The ADM is sutured into place and a bolster applied similar to a skin graft.
The bolster should be kept in place for 3 to 7 days.5
Failure presents as a pale graft that easily sloughs from its wound base.
Mild contraction can occur that is maximal at 3 to 5 weeks.5
▪ Buccal Fat Pad Flap
The body of the buccal fat pad is centrally located over the parotid duct.
The blood supply includes branches of the facial artery, internal maxillary artery, superficial temporal artery, and maxillary artery.
The buccal fat pad can be mobilized to resurface a defect.
Suitable for moderate-sized defects up to 5 cm. Cheek depression can occur in larger defects.6
The flap can be mobilized through a 1-cm horizontal incision in the molar region, 5 mm above the second molar, and halfway between the Stensen duct and the upper gingivobuccal sulcus.Related posts:
 Mandible Reconstruction With Fibula Flap With Templates
Mandible Reconstruction With Fibula Flap With Templates
 Lower Lip Reconstruction With the Nasolabial Flap
Lower Lip Reconstruction With the Nasolabial Flap
 Lateral Tarsal Strip Canthoplasty
Lateral Tarsal Strip Canthoplasty
 Antia-Buch Flaps for Ear Reconstruction
Antia-Buch Flaps for Ear Reconstruction
 Pectoralis Major Flap for Pharyngeal Reconstruction
Pectoralis Major Flap for Pharyngeal Reconstruction
 Facial Reanimation in the Oncologic Patient Using Nerve Grafts and Nerve Transfers
Facial Reanimation in the Oncologic Patient Using Nerve Grafts and Nerve Transfers

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


