Rare Craniofacial Clefts
Justine C. Lee, Henry K. Kawamoto, Jr.
KEY POINTS
○ Craniofacial clefts occur along defined facial axes.
○ Craniofacial clefts can affect all tissue types, including skin, subcutaneous tissue, muscle, nerves, glands, cartilage, and bone.
○ Tissues can be differently affected with varying degrees of severity.
○ Evaluation of the patient with a craniofacial cleft begins with an inventory of all tissues affected.
○ Reconstruction begins with early coverage of vital structures.
○ After protection of vital structures, skeleton restoration precedes soft tissue manipulation.
○ Reconstruction of the craniofacial skeleton and soft tissues are performed with like tissues and attention to the aesthetic subunits.
One of the most deforming conditions of development arises from a conceptually simple disruption of the craniofacial skeleton and soft tissues in a specific three-dimensional space. In the mildest of forms, these disruptions manifest as the common cleft lip or cleft palate. In the most destructive versions, the face becomes a chaotic image with distorted features.
CLASSIFICATION SYSTEMS
The true incidence and prevalence of rare craniofacial clefts are unknown. Estimates range from 1.43 to 4.84 per 10,000 live births.1 Despite their rarity, facial clefts follow certain patterns, and various investigators have sought to devise classification systems to describe such patterns.
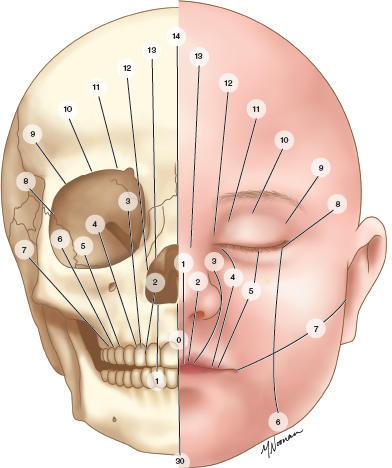
Fig. 52-1 The Tessier classification system of craniofacial clefts: left, skeletal and, right, soft tissue locations of clefts.
The Tessier classification is the most widely used for describing rare craniofacial clefts. It combines clinical experience and surgical observations into a complete and practical system (Fig. 52-1). Using the orbit as the landmark junction between the face and the cranium, clefts are numbered from 0 to 14 and extend along constant axes. Defined skeletal and soft tissue anomalies occur on these axes. Clefts that involve the upper eyelid and travel in a superior direction are termed northbound and are cranial in nature. Clefts that involve the lower eyelid and travel inferiorly are termed southbound and are facial in nature. Combinations of northbound and southbound clefts commonly occur in unison in axes that usually add up to 14. The concept of defined axes is essential in the evaluation of the cleft patient, because it compels the clinician to systematically analyze patients by scanning the entirety of the axis.
APPROACH TO PATIENTS WITH RARE CLEFTS
Before committing the fine anatomic details of each extraordinarily rare cleft to one’s memory, some general principles for approaching rare clefts should be considered. Some of these principles have been adopted from Tessier,2 and others from the compilation of my (H.K.K.) works and experience. These concepts are the following:
• A cleft can differentially affect the quantity of tissue between its edges by allowing:
– Excess tissue to fill the cleft (hyperplasia)
–Normal quantities of tissue (dysraphia)
–An absence of tissue (hypoplasia)
• All clefts have hypoplastic edges; however, hypoplasia is not synonymous with clefting.
• A cleft exists whenever there is any interruption found in the soft tissue (including the hairline, eyebrows, eyelids, nostrils, lips, or ears) or the skeleton.
• Bone and soft tissue are rarely involved to the same extent. From the midline to the infraorbital foramen, defects of the soft tissues and cartilage are more common and destructive than those of the skeleton. From the infraorbital foramen to the temporal bone, defects are more severe in the bone than the soft tissue.
• Clefts are easier to define on the skeleton.
• Clefts are not generally seen along the course of a main vessel.
• Clefts do not traverse foramina.
• Clefts are situated along definite axes.
In addition to Tessier’s principles of the anatomy of clefts, several basic principles in treating rare craniofacial clefts are generally in line with the basic tenets of plastic surgery:
• Early coverage of the globe.
• Early reduction of encephaloceles. Herniation of the brain through cranial clefts not only results in distortion of cranial and facial structures, it causes enlargement of the cleft by providing pressure on the edges.
• Careful planning of the initial soft tissue rearrangement procedure, especially in clefts medial to the infraorbital foramen. Like the cleft lip, soft tissue rearrangement of rare craniofacial clefts should be planned in a manner that adheres to the principle that the first operation dictates the final result. Thus, although virtually all patients with rare craniofacial clefts require multiple operations throughout their lives, the surgeon should plan the initial soft tissue rearrangement as if no other soft tissue operation will be required.
• Reconstruction of compartments to separate various cavities, using autologous or vascularized autologous materials. Unlike adult patients, or patients with specific localized trauma, children with rare craniofacial clefts require repeated interventions and require reconstruction that can ideally survive the lifetime of a patient. Thus the use of materials that are optimally resistant to infection and extrusion is of the greatest importance, and any material that may add to infection risk is not acceptable for use. Furthermore, alloplastic materials cannot grow with the child.
• Attention to the aesthetic subunits of the face for scar placement.
ANATOMIC DESCRIPTIONS OF RARE CLEFTS
Median Clefts: No. 0 and No. 14 Clefts
Median craniofacial clefts occur in the midline of the face and include a spectrum based on tissue quantity ranging from hypoplasia to hyperplasia.3 The No. 0 cleft defines the facial component (Fig. 52-2), and the No. 14 cleft defines the anomalies of the frontoethmoid region (Fig. 52-3). In the mildest of presentations, the median craniofacial cleft may present as minimal hypotelorbitism or mild hypertelorbitism. In the most severe of cases, the brain fails to develop or herniates through midline structures.

Fig. 52-2 The No. 0 midline cleft traverses the lip, alveolus, and nasal structures. The amount of tissue in the midline can range from hypoplasia to normal quantities to hyperplasia.

Fig. 52-3 The No. 14 cleft is the cranial extension of the No. 0 cleft. The frontal sinus and ethmoids are enlarged, and the hypertelorbitism ensues.
Table 52-1 Median Craniofacial Dysplasia Classification
| Median Craniofacial Hypoplasia: Tissue Deficiency or Agenesis | |
| Holoprosencephaly (Alobar Brain) | Lobar Brain |
Cyclopia: single eye in a single orbit; arhinia with proboscis located above the single orbit; microcephaly Ethmocephaly: severe hypotelorism but separate orbits; arhinia with proboscis located between orbits Cebocephaly: severe hypotelorism, proboscis-like rudimentary nose Agenesis of primary palate and associated structures with severe hypotelorism | Median cerebrofacial hypoplasia –Midline cerebral malformation and facial hypoplasia Medial facial hypoplasia – Binder anomaly –Absent central incisor –Absent upper lip frenulum |
| Median Craniofacial Dysraphia: Normal Quantity of Tissue but Clefted | |
| True median cleft Anterior encephalocele | |
| Median Craniofacial Hyperplasia: Tissue Excess or Duplication, Frontonasal Dysplasia | |
Median Craniofacial Hypoplasia
Soft tissue manifestations of median hypoplasia in the No. 0 cleft include median cleft lip, deficiencies of philtral columns, deficiencies of the columella, or deficiencies of the septum. In the most severe cases, arhinia may exist. As it extends cranially as a No. 14 cleft, a decrease in the soft tissue between the eyebrows may occur. Skeletally, the No. 0 cleft can be seen as a spectrum ranging from the lack of one central incisor to a cleft of the alveolus or maxilla. In the No. 14 cleft, the nasal bones may be absent, and the ethmoid sinuses may be underdeveloped.
Patients with median hypoplasia can be divided into those who have holoprosencephaly, or alobar brains, and those with lobar brains (Table 52-1). Four subtypes of holoprosencephaly have been defined: cyclopia, ethmocephaly, cebocephaly, and primary palate agenesis. The severity of the facial anomalies in each subcategory generally correlates to the development of the brain. In contrast, patients with lobar brains usually have a milder median cerebrofacial or facial hypoplasia.
Median Craniofacial Dysraphia
Dysraphia occurs when a normal quantity of tissue in the midline is arranged in an abnormal manner. Dysraphia can be mimicked when herniation of the brain occurs in the midline. In an anterior encephalocele, the herniation does not disrupt the quantity of tissue; however, the tissues are splayed into abnormal spaces.
Median Craniofacial Hyperplasia
Median hyperplasia presents as a widening or duplication of structures. The soft tissue characteristics of the face include broadly separated philtral columns, duplication of the frenulum, or a bifid nose. The nose usually takes on a coarse appearance in median hyperplasia and may demonstrate septal duplication, laterally displaced alar cartilages, a broad columella, and a broad or clefted dorsum.
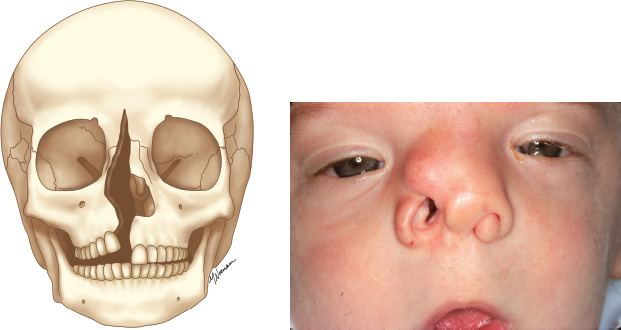
Fig. 52-4 The No. 1 cleft crosses the lip and nose and courses medial to the palpebral fissure. Notching of the soft triangle and disruption of the nasal dome is commonly seen.
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


