Introduction
Drs. Yang and Gao of the Shenyang Military Hospital initially introduced the radial forearm flap, often called the “Chinese flap.” Cadaveric studies performed in 1978 identified this flap and subsequent clinical series published in the Chinese literature in 1981 sealed it as a viable reconstructive option. In 1980, a delegation of German surgeons visiting China saw this flap and subsequently introduced it to the Western world.
The authors of this chapter acknowledge the original chapter contribution by David Soutar.
The initial introduction of this flap was as a free flap in the original 1981 article. It took another year or so for Lu and Biemer to independently reintroduce it as a pedicled flap based on retrograde flow.
Further refinements and delineation of its vascular anatomy increased the reliability and applicability of this flap for local, regional, and distant reconstruction of a variety of defects in the body. The skin is thin and pliable, the vascular anatomy is consistent, and the donor site morbidity is acceptable. It can be sculpted into a sensate flap, adipofascial flap, osteofasciocutaneous flap, or flow-through flap with interposition of vein or artery as a conduit. The forearm provides an ideal location for prelamination of the flap prior to transfer. This flap is the most commonly used fasciocutaneous flap for reconstruction of defects in the head, neck, and limbs. With these versatile qualities, the forearm flap has become one of the most frequently used free tissue transfers.
Flap Anatomy ( Figs 47.1 and 47.2 , See Fig 12.8 , Fig 12.9 , Fig 12.10 , Fig 12.12 , Fig 12.19 , Fig 12.22 , Fig 12.23 )
Arterial Supply of the Flap ( Figs 47.1 and 47.2 and Fig 12.8 , Fig 12.9 , Fig 12.10 )
Dominant ( Figs 47.1 and 47.2 , See Figs 12.8 , 12.9 , 12.10 ):
radial artery
Length: 18.0 cm (range 15.0–22.0 cm) in the adult
Diameter: 3.0 mm (range 2.5–3.5 mm) in the adult
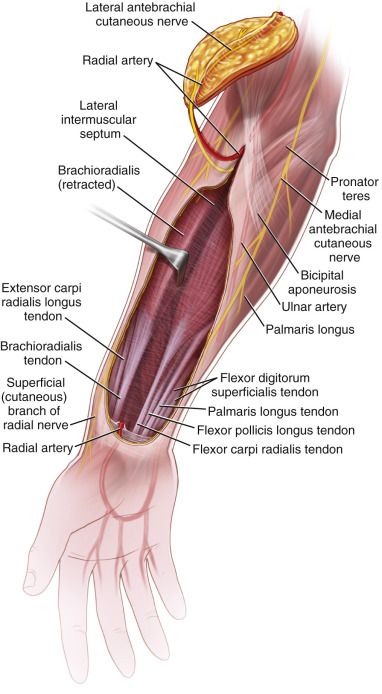
Approximately 12 septocutaneous branches from the radial artery supply the skin of the forearm. Three to four of these branches arise in the proximal forearm between the brachioradialis and the pronator teres muscles ( Fig. 47.2 ). These are large perforators with average diameter >0.5 mm. They supply a large area of skin 4.0 cm below the elbow flexion crease. The rest of the fasciocutaneous perforators are mostly small branches, densely populated in the distal third of the forearm between the tendons of the brachioradialis and flexor carpi radialis. The middle third of the forearm has the lowest density of perforators.

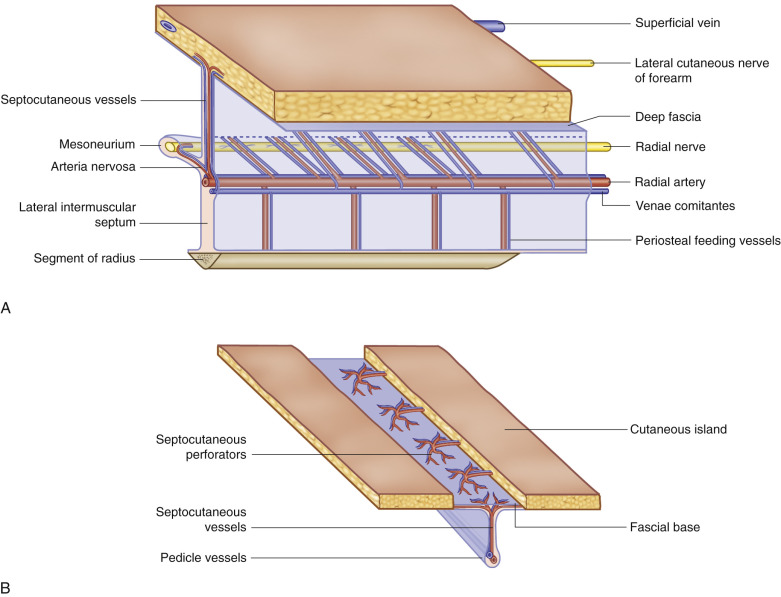
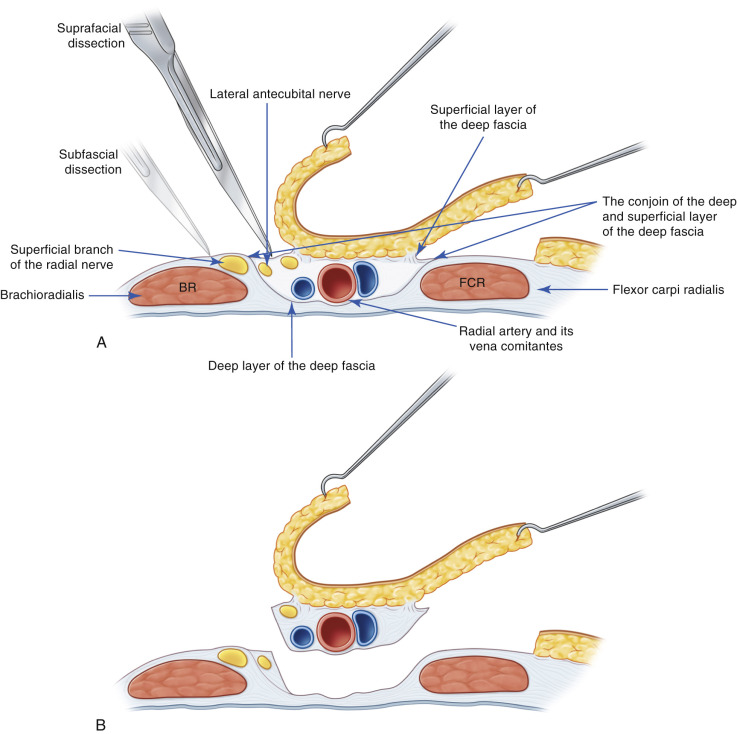
The perforators from the radial artery pass superficial to the deep fascia, and herein, they interconnect to an extensive network of subdermal fascia and vessels ( Fig. 47.3 ). These allow near circumferential vascular nourishment of the forearm, sparing only about a 3.0 cm-wide strip on the ulnar dorsal aspect of the forearm that is not perfused.
Venous Drainage of the Flap (See Figs 12.22 , 12.23 )
Primary:
venae comitantes of the radial artery
Length: 18.0 cm (range 15.0–22.0 cm) in the adult
Diameter: 1.5 mm (range 1.0–2.0 mm) in the adult
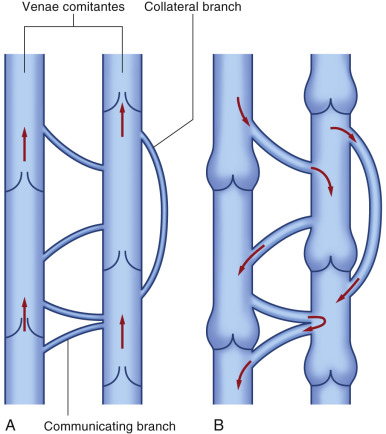
Typically, two venae comitantes follow the radial artery along its course. Connecting these venae comitantes is a plexus of veins devoid of valves that surround the radial artery. Since the venae comitantes contain valves, the connections may be important for drainage of distally based flaps ( Fig. 47.4 ).
Secondary:
cephalic vein (see Fig. 12.19 for superficial veins)
Length: 20.0 cm (range 16.0–24.0 cm) in the adult
Diameter: 3.0 mm (range 2.5–4.0 mm) in the adult
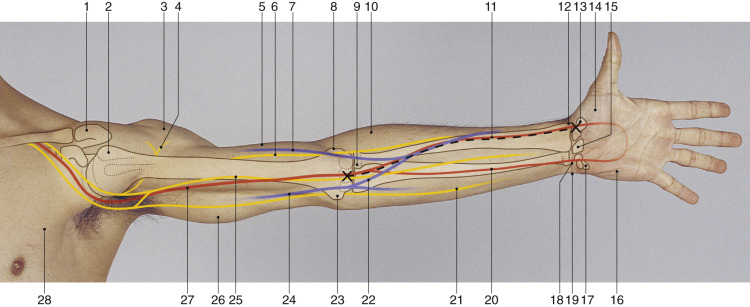
The skin of the forearm flap is drained by a plexus of unnamed superficial veins, many of which empty into the cephalic vein. The cephalic vein can be dissected proximally the whole length of the arm up to the deltopectoral groove. It can be used as extra venous drainage for the flap, or as a conduit for reconstructing the radial artery in reverse flow flaps.
Flap Innervation (see Fig 12.19 , Fig 12.22 )
Sensory
- •
Lateral antebrachial cutaneous nerve: innervates the lateral (radial) half of the volar surface of the forearm
- •
Medial antebrachial cutaneous nerve: innervates the medial (ulnar) half of the volar surface of the forearm
Flap Components
In addition to the skin, fat, and fascia, this septocutaneous flap can be raised containing vascularized nerve, tendon (palmaris longus, brachioradialis, flexor carpi radialis), and bone incorporating a segment of the distal radius ( Fig. 47.3 ). Given the importance of the flexor muscle compartment for the function of the hand, this flap does not typically incorporate any functional muscle components.
Advantages
- •
The flap has reliable vascular anatomy.
- •
The radial artery and its venae comitantes are large in diameter and microanastomoses are more predictable.
- •
Substantial pedicle length can be obtained, thus the flap can reach difficult areas such as the palate, the skull base, pharynx, or interdigital spaces.
- •
The artery and/or its veins can be used as interpositional grafts and the flap can be used as a flow-through flap (see Case 47.4 ).
- •
There is flexibility of venous anastomosis due to extensive redundancy of veins.
- •
The flap can be free, pedicled, distally based, or proximally based.
- •
A combination of tissues can be harvested, including skin, fat, fascia, nerve, tendon, and bone.
- •
Very small to very large flaps can be harvested reliably.
- •
The skin is thin, pliable, and in many individuals, hairless.
- •
The flap can be harvested under regional block.
Disadvantages
- •
The donor site is in a conspicuous location.
- •
Unless a very small flap is harvested, the donor site usually requires a skin graft for closure.
- •
Healing of the skin graft can be delayed if the fascia over the flexor carpi radialis is taken.
- •
Secondary fractures may occur when large osseous segments are harvested, particularly in the elderly.
- •
The flap requires sacrifice of a major artery of the forearm and hand (unless revascularized).
Preoperative Preparation
It is common practice to choose the donor site from the nondominant arm. The ulnar and radial arteries must be assessed for patency via physical examination. An Allen test can ensure that the hand will remain well-perfused after division of the radial artery. Although a traditional Allen test relies on clinical visualization, a more reliable test uses a pulse oximeter probe on the thumb. The thumb is the most distal digit to be perfused by the ulnar artery via a patent arch. Once pressure on the ulnar artery is relieved (while holding continued pressure on the radial artery), one should see return of waveform and strong oximetry signal within 5 s. A substantial delay in return of the waveform or a dampened waveform should alert the surgeon about the possibility of an incomplete arch. In these cases, one option is to place a clamp on the radial artery and reperfuse the hand before dividing the radial artery to make sure that the hand becomes perfused. The other option is to plan a priori to reconstruct the radial artery defect with a reversed vein graft, or to avoid the flap altogether. Preoperative vascular imaging is rarely needed but helpful following extensive trauma, congenital malformations, electrical and thermal burns, and conditions such as purpura fulminans.
If the bone is to be taken, preoperative plain films should be obtained for planning and to ensure that there is no pathology.
Flap Design
Anatomic Landmarks
Although nearly all of the forearm skin can be taken as a free flap based on the radial artery angiosome, this would be highly morbid because of the disruption of the lymphatic drainage from the hand. In practice, a strip of skin at least 3.0–5.0 cm in width overlying the posterior extensor compartment and the ulnar subcutaneous border should be kept intact at a minimum.
The path of the radial artery is marked by drawing a line from 1.0 cm distal to the midline of the elbow flexion crease to the scaphoid tubercle (see Fig. 47.5 ). The artery is easily palpable in the distal forearm and can be followed well into its middle third with a Doppler probe.
Proximal pressure above the elbow helps to engorge veins in the forearm and make them visible for marking and incorporation into the flap design.
General Considerations
Smaller flaps should be designed in the distal third of the forearm to ensure proper incorporation of perforators. The skin and subcutaneous tissue here can be quite thin. A suprafascial dissection can be performed ulnar and radial to the artery and then taken deep to the fascia as the artery is approached ( Fig. 47.6 ). This technique protects the tendons from exposure, preserves the epitendinous connective tissue, and enhances skin graft take. Very small, distally situated donor sites can usually be closed with skin advancement.
Flaps harvested from the center of the forearm harbor the fewest perforators. These should be larger flaps to avoid missing perforators. In these situations, it is advisable to take a large cuff of fascia to ensure capture of as many perforators as possible ( Fig. 47.7 ).
Proximally designed flaps are thicker, as they have more subcutaneous fat. Small flaps designed proximally can be problematic because there are fewer perforators and there is risk that a perforator may not be incorporated in the flap. Subfascial dissection is important to preserve perforators, which are more widely spaced in this area. Antegrade flaps designed proximally are not typically used because the pedicle length is shorter, the vascularity less reliable (due to fewer perforators), and the flap thicker and less pliable.
Special Considerations
Flaps that will be used as skin tubes need to be broad and usually incorporate all of the volar aspects of the forearm. When used for reconstruction of the cervical esophagus, ideally the upper and lower ends can be angulated, so that the ends become wide (cone-shaped). Flaps for penile reconstruction need substantial width due to the need for creation of a urethra, an area of de-epithelialized skin, and an area for forming the outer surface of the penis (see Case 47.3 ).
If bone is incorporated, only the distal part of the radius between the pronator teres and the radial styloid is accessible and well-vascularized. The maximum length of bone that can be harvested in most instances is 12.0 cm. Harvesting more bone, however, is inadvisable because it may result in the need to provide coverage for the bone, and/or may weaken the radius substantially and increase the likelihood of fracture. The authors advise against incorporating the radius unless a small segment of bone is needed. Alternative donor sites can provide a substantial amount of well-vascularized bone with far less morbidity. These include the medial femoral condyle or the fibular flaps. If a segment of bone 5 cm or larger is taken from the radius, we recommend bone grating and plate fixation.
Design Differences in Free Versus Pedicled Flaps
Distal flap design is identical for free and pedicled flaps. Distally designed pedicled flaps are ideal for reconstruction around the elbow or arm. Proximal forearm flaps are most commonly used as pedicled reverse-flow flaps for hand and digit reconstruction.
Flap Dimensions
Skin Island Dimensions
Length: 12.0 cm (range 4.0–30.0 cm) in the adult
Width: 5.0 cm (range 4.0–15.0 cm) in the adult
Maximum width to close primarily: 1.0–2.0 cm, but dependent on the flap donor site location on the forearm
Thickness: 1.0 cm (range 0.5–2.0 cm, but dependent on where the skin is harvested – thinner distally)
Bone Dimensions
Length: 10.0 cm (range 6.0–14.0 cm) in the adult
Width: 1.0 cm (range 0.7–1.5 cm) in the adult
Thickness: 1.0 cm (range 0.7–1.5 cm) in the adult
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


