Acne vulgaris affects most adolescents and two-thirds of adults and is associated with substantial psychosocial burden. Health-related quality of life (HRQOL) for patients with acne is an important factor of patient care, and several dermatologic and acne-specific measures have been created to assist in acne research, management, and care. This review describes several skin disease and acne-specific HRQOL measures and their applications in clinical care or research. The ideal HRQOL measure for the management of patients with acne is a concise questionnaire that places minimal burden on respondents and allows physicians to track improvement in HRQOL with successful treatment.
Acne vulgaris is a chronic condition affecting more than 85% of adolescents and two-thirds of adults aged 18 years and older. Adolescents aged 15 to 17 years are the most represented of patients with acne; however, as the age of onset approaches as early as 8 or 9 years and a substantial portion of patients experience this condition in adulthood, addressing acne comorbidities and quality of life is gaining importance. Although no correlation exists between acne severity and psychological burden, acne patients may experience psychological burdens. including depression, anxiety, and lower self-esteem. Acne focus groups report social avoidance; feelings of anger, sadness, or frustration; and the development of negative attitudes. Furthermore, acne episodes produce a financial burden on patients; the cost of an acne episode averages $690 and ranges from $360 to $870, covering inpatient stays, outpatient services, emergency care, and pharmacy costs during the episode.
Health-related quality of life (HRQOL) refers to the physical, psychological, and social well-being an the emotional, physical, and social functioning reported by patients. Current acne therapy often involves the assessment of HRQOL from the negative impact acne can have on a patient’s functioning. For example, facial blemishes in women are correlated with lower HRQOL and fear of negative perceptions; the simple presence of a facial blemish, and not just the type or size of blemishes, contributes to lower HRQOL in women. Quality of life improves as acne clears with successful treatment. Treatment may have an even greater effect on improving HRQOL in patients with depressive symptoms at the outset of treatment.
The use of HRQOL assessments in clinical practice provides physicians with valuable insight into the debilitating effects of acne that patients may not address themselves. One can determine the present psychosocial effects of acne on a patient and also track changes and improvements in HRQOL easily in the clinical setting. Several dermatology-specific and acne-specific HRQOL questionnaires have been developed and vary in both the number and content of items addressing quality of life. A longer questionnaire may better serve clinical trial visits, yet can also provide a more comprehensive profile of patients’ HRQOL than a brief measure. This review explores several formal skin disease–specific and acne-specific HRQOL measures to determine the most beneficial use of these assessments. The review also briefly explores the psychological comorbidities in patients with acne; the risk factors for low quality-of-life scores; and recommendations for physician intervention to improve HRQOL.
Methods
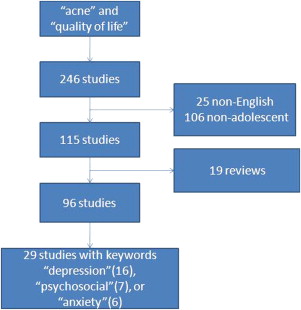
A MEDLINE literature search was performed using the key words acne and quality of life . The 246 resulting studies were limited to the English language and adolescents aged 13 to 18 years, which produced 115 studies. Adults older than 18 years can also have acne; however, adolescents are the most represented of patients and this review focuses on this age group. Nineteen reviews were eliminated, and the search was further narrowed using the keywords depression , psychosocial , and anxiety . Twenty-nine studies pertaining to acne quality-of-life indices and scales were reviewed ( Fig. 1 ).
Results
General Dermatology HRQOL Measures
Physicians and researchers use HRQOL measures to assess the emotional, psychological, and social effects of disease on patients’ lives. General HRQOL measures provide a means of comparing effects of different conditions on patients’ lives. Skin disease–specific measures address the effects of multiple types of skin disease and offer a more sensitive HRQOL measure than a generic health questionnaire.
Finlay and Khan developed the widely used Dermatology Life Quality Index (DLQI) for use in research studies and routine clinical practice. The details of the DLQI are discussed in the article by Basra and colleagues which is addressed elsewhere in this issue. The DLQI can be used in clinical practice to assess changes in HRQOL and is meant to provide a sensitive measure of patient HRQOL that streamlines its assessment for multiple dermatologic conditions. The DLQI has been modified for pediatric dermatology HRQOL (Children’s DLQI) and to assess the secondary effects of a dermatologic condition on the patients’ family (Family DLQI). Application of the DLQI in acne shows that scores are lower in these patients than in those with atopic eczema, generalized pruritus, and psoriasis, yet were significantly higher than those for Finlay’s control population. The difference in scores can be attributed to the absence of items addressing depressive or anxious feelings; only 1 item of the 10 concerns the amount of embarrassment or self-consciousness experienced by the patient as a result of their skin condition. The DLQI item addressing the extent of the patient’s itchiness, soreness, or pain is less applicable to patients with acne, which contributes to these patients’ less-severe scores compared with patients with psoriasis or eczema.
The Skindex is another comprehensive dermatologic disease HRQOL measure developed by Chren and colleagues and also discussed in detail in the article by Chren elsewhere in this issue. Skindex scores for patients with different dermatologic conditions varied; average scores for patients with inflammatory conditions such as acne, eczema, and psoriasis were higher than those for patients with isolated lesions. Patients with inflammatory conditions such as acne, eczema, or psoriasis had lower HRQOL scores than patients with isolated skin lesions. Acne patients’ judgments of their acne severity correlated with both the physical limitation and embarrassment scales. Nijsten and colleagues used the Skindex-29 to categorize patient scores and examine whether scores differed among patients with acne, psoriasis, seborrheic dermatitis, alopecia areata, vitiligo, and nevi. Skindex-29 scores were categorized into emotions, symptoms, and functioning items. A higher percentage of acne patients ranked their emotions items as “moderate” or “severe” compared with psoriasis patients, yet a higher percentage of patients with psoriasis ranked their functioning and symptoms items as “moderate,” “severe,” or “extremely severe.” Skindex supports a greater emotional and psychosocial burden of acne on patients compared with other inflammatory diseases like psoriasis.
Dermatology Quality of Life Scales (DQOLS) were developed by Morgan and colleagues to complement the scores of Finlay’s DLQI and focus on the psychosocial burden of dermatologic diseases. Morgan’s DQOLS incorporates the impact of a dermatologic condition on patients’ psychosocial burden and daily activities, with items generated by patients reporting on their psoriasis, acne, or eczema. Seventeen psychosocial items are categorized into four subscales (embarrassment, despair, irritableness, and distress); the 12 daily activities items fall into one of four subscales (everyday, summer, social, and sexual). The DQOLS offer a patient-generated measure of the impact of skin conditions such as psoriasis, eczema, and acne. Patients with acne scored higher in the psychosocial categories than those with psoriasis or eczema, indicating that acne has a greater psychosocial impact than psoriasis. This finding was exemplified by 36% of patients with acne and 26% of those with psoriasis reporting their skin condition “extremely” affecting how they felt regarding the despair items (lack of hope, lack of understanding from others, isolated, worry about long-term effects, or ashamed). A greater number of patients with acne (24%) than those with psoriasis (21%) also rated their skin condition as “extremely” affecting their feelings about the distress items (suicidal, anxious, depressed, or distressed). Acne did not, however, have as great an effect on daily activities as psoriasis. The greater number of psychosocial items specifically addressed on the DQOLS lends to its usefulness in assessing the psychological impact of acne.
Niemeier and colleagues evaluated the use of the Questionnaire of Chronic Skin Disorders (CSD) in patients with acne, which examines six aspects of coping behaviors in individuals with chronic skin diseases. The aspects include social anxiety and avoidance; cycle of itching and scratching; helplessness; anxious-depressive mood; impact on quality of life; and information seeking. Each of the six dimensions is a subscale of the CSD with a higher score, indicating lower HRQOL. Patients with acne had higher scores on every CSD subscale except the anxious-depressive mood subscale, and CSD scores were independent of the duration of patient symptoms. The CSD subscales correlated significantly with Beck’s Depression Inventory (BDI) and indicated that, compared with patients with pain or depressive, patients with acne had depressive scores similar to healthy persons. Although Niemeier and colleagues assessed the validity of the CSD in patients with acne, it can be used to compare different skin conditions, various presentations of acne, and methods of acne therapy.
Acne-Specific Health-Related Measures
Although skin disease quality-of-life indices and questionnaires serve the purpose of gauging the impact of dermatologic conditions on a patient’s life and comparing the impacts of different skin diseases, an acne-specific HRQOL assessment can offer a focused examination of the negative effects of acne. An acne-focused HRQOL measure is the most sensitive way to determine the impact of acne and allows the dermatologist to assess the effects of acne on patients while excluding irrelevant symptoms.
The Acne Quality of Life Index (Acne-QOLI) is a 21-item measure covering three conceptual domains of HRQOL: social functioning, psychological functioning, and emotional functioning. The scale has very good internal consistency and excellent test–retest reliability and validity. The Acne-QOLI is advantageous for use in clinical trials and everyday clinic operations, and offers a comprehensive yet concise analysis of the HRQOL of patients with acne. The 21 items cover a range of emotional and social effects of acne, including feeling uncomfortable, angry, unattractive to others, and wanting to avoid people, and 17 additional patient-reported feelings associated with acne. The Acne-QOLI does not include acne severity or treatment items, and therefore avoids respondent confounding and provides a simple and effective measure of acne’s negative effects on the patient. The length of the Acne-QOLI is not a major burden on respondents, and potentially could be incorporated into a routine clinic visit.
The Cardiff Acne Disability Index (CADI) was developed to quickly assess the level of disability caused by acne and to identify patients with increased disability and the need for additional intervention. Health-related disability refers to any restriction or inability to perform an activity within the normal range of human ability. The CADI is a condensed version of the Acne Disability Index (ADI), which consists of 48 items in eight HRQOL domains (psychological, physical, recreation, employment, self-awareness, social reaction, skin care, and financial). The CADI consists of five questions, each with four graded responses, pertaining to disability caused by acne in the past month and addresses general psychological and social burdens of acne and the respondent’s perception of the severity of their facial, chest, and back acne, if applicable. Motley and Finlay intended for the CADI to assess a patient’s disability from acne and to identify patients who may benefit from psychological interventions in addition to acne therapy. Salek and colleagues showed the validity of the CADI compared with ADI and a generic HRQOL measure, the United Kingdom Sickness Impact Profile (UKSIP), and determined that the CADI is more appropriate for routine clinical use and monitoring the HRQOL of patients with acne. The CADI has been widely used and has been translated and adapted into French, Chinese, and Persian versions.
The Acne-QoL is a 24-item questionnaire specific to facial acne in which the questions are organized into four domains: self-perception, role-emotional, role-social, and acne symptoms. Each question refers to the previous week of treatment for facial acne, thus allowing dermatologists to detect improvement over the course of therapy. The Acne-QoL, which can be condensed into a 19-item questionnaire through eliminating five redundant items, is estimated to require 5 to 7 minutes to complete and offers a comprehensive score encompassing the psychosocial burden of facial acne. Quality-of-life scores correlated strongly with patient-reported acne severity, more so than with physician-reported severity. The Acne-QoL is a comprehensive assessment of patient-perceived acne severity; however, it addresses facial acne exclusively, and the extended time requirement to complete the questionnaire makes the Acne-QoL more useful in clinical trials than in the everyday clinic.
Tan and colleagues condensed the 19-item Acne-QoL into a 4-item questionnaire (Acne-Q 4 ), including the highest-ranked items from each of the four domains from the Acne-QoL. The four items include “Dissatisfied with appearance” (self-perception), “Feeling upset” (role-emotional), “Concern about meeting new people” (role-social), and “Concern about scarring from facial acne” (acne symptoms). The Acne-Q 4 was a good predictor of Acne-QoL score and also exhibited a relationship with physician-rated Investigators Global Assessment (IGA) scores of facial acne severity. The Acne-Q 4 shares the Acne-QoL restriction to facial acne and is not applicable to patients with truncal acne or minimal facial acne. Although the Acne-Q 4 is restricted to use with facial acne and does not offer the breadth of quality-of-life information, it is a practical substitution for the Acne-QoL in clinical practice.
An Acne Quality of Life scale (AQOL) was developed by Gupta and colleagues to specifically address the social and occupational functioning aspects of quality of life. This 12-item scale can be divided into two subscales, social quality of life (9 items) and vocational quality of life (3 items), although the 9 social quality-of-life items constitute the final version of the AQOL. Social scores correlate significantly with Interpersonal Dependency Inventory (IDS), Carroll Rating Scale for Depression (CRSD), and other psychopathologic scales; thus, the AQOL serves as an accurate psychological measure for patients without serious psychopathology. Respondents completed the AQOL in less than 5 minutes, indicating potential ease of use in the routine clinical setting.
For patients with signs of a psychological comorbidity such as depression, the Assessment of the Psychological and Social Effects of Acne (APSEA) is an effective 15-item psychological-specific measure. The APSEA was used in a study examining the psychological changes in patients with acne treated with oral isotretinoin. APSEA scores in patients taking isotretinoin for acne correlated with Beck’s Depression Inventory (BDI) scores, which address the cognitive, affective, and physical symptoms of depression. APSEA scores and acne severity improved in patients after 8 weeks of treatment, suggesting that APSEA scores are responsive to clinical change. Hahm and colleagues suggest that skin clearance from oral isotretinoin treatment can improve HRQOL, which in turn improves and reduces depressive symptoms. An acne-specific psychological assessment is an important tool to measure changes in HRQOL for patients with preexisting psychological symptoms, and APSEA provides an efficient clinical alternative to an in-depth psychological assessment.
Results
General Dermatology HRQOL Measures
Physicians and researchers use HRQOL measures to assess the emotional, psychological, and social effects of disease on patients’ lives. General HRQOL measures provide a means of comparing effects of different conditions on patients’ lives. Skin disease–specific measures address the effects of multiple types of skin disease and offer a more sensitive HRQOL measure than a generic health questionnaire.
Finlay and Khan developed the widely used Dermatology Life Quality Index (DLQI) for use in research studies and routine clinical practice. The details of the DLQI are discussed in the article by Basra and colleagues which is addressed elsewhere in this issue. The DLQI can be used in clinical practice to assess changes in HRQOL and is meant to provide a sensitive measure of patient HRQOL that streamlines its assessment for multiple dermatologic conditions. The DLQI has been modified for pediatric dermatology HRQOL (Children’s DLQI) and to assess the secondary effects of a dermatologic condition on the patients’ family (Family DLQI). Application of the DLQI in acne shows that scores are lower in these patients than in those with atopic eczema, generalized pruritus, and psoriasis, yet were significantly higher than those for Finlay’s control population. The difference in scores can be attributed to the absence of items addressing depressive or anxious feelings; only 1 item of the 10 concerns the amount of embarrassment or self-consciousness experienced by the patient as a result of their skin condition. The DLQI item addressing the extent of the patient’s itchiness, soreness, or pain is less applicable to patients with acne, which contributes to these patients’ less-severe scores compared with patients with psoriasis or eczema.
The Skindex is another comprehensive dermatologic disease HRQOL measure developed by Chren and colleagues and also discussed in detail in the article by Chren elsewhere in this issue. Skindex scores for patients with different dermatologic conditions varied; average scores for patients with inflammatory conditions such as acne, eczema, and psoriasis were higher than those for patients with isolated lesions. Patients with inflammatory conditions such as acne, eczema, or psoriasis had lower HRQOL scores than patients with isolated skin lesions. Acne patients’ judgments of their acne severity correlated with both the physical limitation and embarrassment scales. Nijsten and colleagues used the Skindex-29 to categorize patient scores and examine whether scores differed among patients with acne, psoriasis, seborrheic dermatitis, alopecia areata, vitiligo, and nevi. Skindex-29 scores were categorized into emotions, symptoms, and functioning items. A higher percentage of acne patients ranked their emotions items as “moderate” or “severe” compared with psoriasis patients, yet a higher percentage of patients with psoriasis ranked their functioning and symptoms items as “moderate,” “severe,” or “extremely severe.” Skindex supports a greater emotional and psychosocial burden of acne on patients compared with other inflammatory diseases like psoriasis.
Dermatology Quality of Life Scales (DQOLS) were developed by Morgan and colleagues to complement the scores of Finlay’s DLQI and focus on the psychosocial burden of dermatologic diseases. Morgan’s DQOLS incorporates the impact of a dermatologic condition on patients’ psychosocial burden and daily activities, with items generated by patients reporting on their psoriasis, acne, or eczema. Seventeen psychosocial items are categorized into four subscales (embarrassment, despair, irritableness, and distress); the 12 daily activities items fall into one of four subscales (everyday, summer, social, and sexual). The DQOLS offer a patient-generated measure of the impact of skin conditions such as psoriasis, eczema, and acne. Patients with acne scored higher in the psychosocial categories than those with psoriasis or eczema, indicating that acne has a greater psychosocial impact than psoriasis. This finding was exemplified by 36% of patients with acne and 26% of those with psoriasis reporting their skin condition “extremely” affecting how they felt regarding the despair items (lack of hope, lack of understanding from others, isolated, worry about long-term effects, or ashamed). A greater number of patients with acne (24%) than those with psoriasis (21%) also rated their skin condition as “extremely” affecting their feelings about the distress items (suicidal, anxious, depressed, or distressed). Acne did not, however, have as great an effect on daily activities as psoriasis. The greater number of psychosocial items specifically addressed on the DQOLS lends to its usefulness in assessing the psychological impact of acne.
Niemeier and colleagues evaluated the use of the Questionnaire of Chronic Skin Disorders (CSD) in patients with acne, which examines six aspects of coping behaviors in individuals with chronic skin diseases. The aspects include social anxiety and avoidance; cycle of itching and scratching; helplessness; anxious-depressive mood; impact on quality of life; and information seeking. Each of the six dimensions is a subscale of the CSD with a higher score, indicating lower HRQOL. Patients with acne had higher scores on every CSD subscale except the anxious-depressive mood subscale, and CSD scores were independent of the duration of patient symptoms. The CSD subscales correlated significantly with Beck’s Depression Inventory (BDI) and indicated that, compared with patients with pain or depressive, patients with acne had depressive scores similar to healthy persons. Although Niemeier and colleagues assessed the validity of the CSD in patients with acne, it can be used to compare different skin conditions, various presentations of acne, and methods of acne therapy.
Acne-Specific Health-Related Measures
Although skin disease quality-of-life indices and questionnaires serve the purpose of gauging the impact of dermatologic conditions on a patient’s life and comparing the impacts of different skin diseases, an acne-specific HRQOL assessment can offer a focused examination of the negative effects of acne. An acne-focused HRQOL measure is the most sensitive way to determine the impact of acne and allows the dermatologist to assess the effects of acne on patients while excluding irrelevant symptoms.
The Acne Quality of Life Index (Acne-QOLI) is a 21-item measure covering three conceptual domains of HRQOL: social functioning, psychological functioning, and emotional functioning. The scale has very good internal consistency and excellent test–retest reliability and validity. The Acne-QOLI is advantageous for use in clinical trials and everyday clinic operations, and offers a comprehensive yet concise analysis of the HRQOL of patients with acne. The 21 items cover a range of emotional and social effects of acne, including feeling uncomfortable, angry, unattractive to others, and wanting to avoid people, and 17 additional patient-reported feelings associated with acne. The Acne-QOLI does not include acne severity or treatment items, and therefore avoids respondent confounding and provides a simple and effective measure of acne’s negative effects on the patient. The length of the Acne-QOLI is not a major burden on respondents, and potentially could be incorporated into a routine clinic visit.
The Cardiff Acne Disability Index (CADI) was developed to quickly assess the level of disability caused by acne and to identify patients with increased disability and the need for additional intervention. Health-related disability refers to any restriction or inability to perform an activity within the normal range of human ability. The CADI is a condensed version of the Acne Disability Index (ADI), which consists of 48 items in eight HRQOL domains (psychological, physical, recreation, employment, self-awareness, social reaction, skin care, and financial). The CADI consists of five questions, each with four graded responses, pertaining to disability caused by acne in the past month and addresses general psychological and social burdens of acne and the respondent’s perception of the severity of their facial, chest, and back acne, if applicable. Motley and Finlay intended for the CADI to assess a patient’s disability from acne and to identify patients who may benefit from psychological interventions in addition to acne therapy. Salek and colleagues showed the validity of the CADI compared with ADI and a generic HRQOL measure, the United Kingdom Sickness Impact Profile (UKSIP), and determined that the CADI is more appropriate for routine clinical use and monitoring the HRQOL of patients with acne. The CADI has been widely used and has been translated and adapted into French, Chinese, and Persian versions.
The Acne-QoL is a 24-item questionnaire specific to facial acne in which the questions are organized into four domains: self-perception, role-emotional, role-social, and acne symptoms. Each question refers to the previous week of treatment for facial acne, thus allowing dermatologists to detect improvement over the course of therapy. The Acne-QoL, which can be condensed into a 19-item questionnaire through eliminating five redundant items, is estimated to require 5 to 7 minutes to complete and offers a comprehensive score encompassing the psychosocial burden of facial acne. Quality-of-life scores correlated strongly with patient-reported acne severity, more so than with physician-reported severity. The Acne-QoL is a comprehensive assessment of patient-perceived acne severity; however, it addresses facial acne exclusively, and the extended time requirement to complete the questionnaire makes the Acne-QoL more useful in clinical trials than in the everyday clinic.
Tan and colleagues condensed the 19-item Acne-QoL into a 4-item questionnaire (Acne-Q 4 ), including the highest-ranked items from each of the four domains from the Acne-QoL. The four items include “Dissatisfied with appearance” (self-perception), “Feeling upset” (role-emotional), “Concern about meeting new people” (role-social), and “Concern about scarring from facial acne” (acne symptoms). The Acne-Q 4 was a good predictor of Acne-QoL score and also exhibited a relationship with physician-rated Investigators Global Assessment (IGA) scores of facial acne severity. The Acne-Q 4 shares the Acne-QoL restriction to facial acne and is not applicable to patients with truncal acne or minimal facial acne. Although the Acne-Q 4 is restricted to use with facial acne and does not offer the breadth of quality-of-life information, it is a practical substitution for the Acne-QoL in clinical practice.
An Acne Quality of Life scale (AQOL) was developed by Gupta and colleagues to specifically address the social and occupational functioning aspects of quality of life. This 12-item scale can be divided into two subscales, social quality of life (9 items) and vocational quality of life (3 items), although the 9 social quality-of-life items constitute the final version of the AQOL. Social scores correlate significantly with Interpersonal Dependency Inventory (IDS), Carroll Rating Scale for Depression (CRSD), and other psychopathologic scales; thus, the AQOL serves as an accurate psychological measure for patients without serious psychopathology. Respondents completed the AQOL in less than 5 minutes, indicating potential ease of use in the routine clinical setting.
For patients with signs of a psychological comorbidity such as depression, the Assessment of the Psychological and Social Effects of Acne (APSEA) is an effective 15-item psychological-specific measure. The APSEA was used in a study examining the psychological changes in patients with acne treated with oral isotretinoin. APSEA scores in patients taking isotretinoin for acne correlated with Beck’s Depression Inventory (BDI) scores, which address the cognitive, affective, and physical symptoms of depression. APSEA scores and acne severity improved in patients after 8 weeks of treatment, suggesting that APSEA scores are responsive to clinical change. Hahm and colleagues suggest that skin clearance from oral isotretinoin treatment can improve HRQOL, which in turn improves and reduces depressive symptoms. An acne-specific psychological assessment is an important tool to measure changes in HRQOL for patients with preexisting psychological symptoms, and APSEA provides an efficient clinical alternative to an in-depth psychological assessment.
Related posts:
 Health-Related Quality of Life in Dermatology: Introduction and Overview
Overview of Health Status Quality-of-Life Measures
Quality-of-Life Issues in Vitiligo
Melasma Quality of Life Measures
Clinical Meaning in Skin-specific Quality of Life Instruments: A Comparison of the Dermatology Life Quality Index and Skindex Banding Systems
Future Directions in Dermatology Quality of Life Measures
Health-Related Quality of Life in Dermatology: Introduction and Overview
Overview of Health Status Quality-of-Life Measures
Quality-of-Life Issues in Vitiligo
Melasma Quality of Life Measures
Clinical Meaning in Skin-specific Quality of Life Instruments: A Comparison of the Dermatology Life Quality Index and Skindex Banding Systems
Future Directions in Dermatology Quality of Life Measures
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


