60 Quality Control and Quality Assurance during the Follicular Unit Excision Process
Summary
Keywords: quality control quality assurance transection injuries paring missing graft
Key Points
•Quality control is a crucial step that every surgeon must integrate into their practice.
•The principal enemies of regrowth are mechanical damage and dehydration of the follicle suffered during the excision and implantation process.
•The implementation of quality control practices requires time and dedicated personnel. This likely explains why quality control is not widespread in hair transplant practice.
•However, the observation of quality control practices is highly worthwhile and will have a rapid effect on the success of surgeries.
60.1 Introduction
Quality control is a set of practices focused on creating a quality finished product or results. For hair transplantation, it essentially requires control of graft quality throughout all the steps of the follicular unit excision (FUE) procedure in order to obtain optimal hair regrowth.
Quality assurance focuses on the process. It consists of defining the best rules and protocols to put in place in order to prevent procedural defects and obtain the highest quality product possible.
The objective of quality control and assurance is to obtain consistent high-quality results, by following and monitoring established rules and protocols and detecting when deficiencies appear.
With respect to FUE, quality control is particularly important due to the intrinsic difficulty of obtaining high-quality grafts and good survival. FUE grafts are inherently more fragile than those obtained through follicular unit transplantation (FUT) as they have less protective tissue surrounding the follicular stems. Therefore, they are a priori more likely to be damaged during excision, storage, or implantation.
60.2 Why is Quality Control Underdeveloped?
Quality control for FUE requires the systematic measurement of both pre- and intraoperative factors that can maximize donor supply, graft survival, and results. Preoperative parameters to measure include the size of the recipient and donor areas, donor density, hair density, hair caliber, and predicted hair/graft, etc. Intraoperative parameters to follow include graft transection rate, missed graft rates, average hair/per graft, and more. The results of these data will be used to alter the surgical plan preoperatively or adjust surgical technique intraoperatively to achieve maximum survival and best results.
The author became aware very early on of the difficulties in monitoring these parameters in order to obtain good FUE grafts (Fig. 60.1). To this end, the author developed an Excel table (Table 60.1) that quickly calculates the main indexes, allowing him to judge the quality of his work. Other physicians have other means of evaluating similar parameters.

Fig. 60.1 Good follicular unit excision (FUE) grafts with a low rate of transection, and with the least damage possible.
Table 60.1 Photo of Excel spreadsheet used by the author that quickly and automatically lets him calculate important graft parameters
This is quite obviously a time-consuming undertaking and can take one to two staff members who are dedicated solely to follicular unit (FU) quantification. Some of these parameters can only be measured with precise stereomicroscopes, which many physicians who do exclusively FUE do not have. These are just a few of the reason why quality control is often not done well in many clinics.
In addition, evaluating your results is another important component of quality control. You need to know your results in order to know when your technique needs to be adjusted. However, this too can be difficult for many reasons. A few reasons include poor patient follow-up, long time between procedure and results, simultaneous progression of hair loss and graft growth, and the unknown contribution of medications, which can alter hair density.
60.3 Important Elements to Follow and Verify
The different steps of the FUE procedure in which the viability of the grafts may be jeopardized are, in order of succession, the following: excision, storage, implantation, and postoperative care.
60.3.1 Graft Excision
Excision techniques are numerous: manual or motorized, with or without suction, and using sharp, blunt, or hybrid punches. They are each characterized by different risks.
There are two main phases to the FUE: (1) the incision phase, which involves scoring the epidermis, followed by dissection of the dermis with a punch, and (2) the extraction phase, which involves removing the incised graft from the skin. Both involve risk of graft damage.
Incision Phase (Scoring and Dissection)
It is important to count the total number of punch insertions and the number of grafts actually obtained. The number of missing grafts is calculated: this is the difference between the number of punch insertions or attempts and the number of grafts actually extracted. Missing grafts include buried grafts, complete follicle transections left on the operative field, or simply a counting error. Missing graft rate should ideally be less than 5%.
Excision is the time during which mechanical damage is potentially the greatest. A list of the possible injuries that can occur are described and defined in Chapter 52.1,2 These include paring, broken grafts, plucked grafts, and, of course, transections themselves (Fig. 60.2). They should be counted for the first 100 or, better still, 200 to 300 grafts. It is preferable to count quickly so that the parameters of the FUE procedure can be modified if necessary. Such modifications might include changing the depth of the punch insertion or the diameter of the punch. It is also important to note these parameters in order to draw conclusions over the long term and compare, for example, the effectiveness of a certain type of punch or technique.
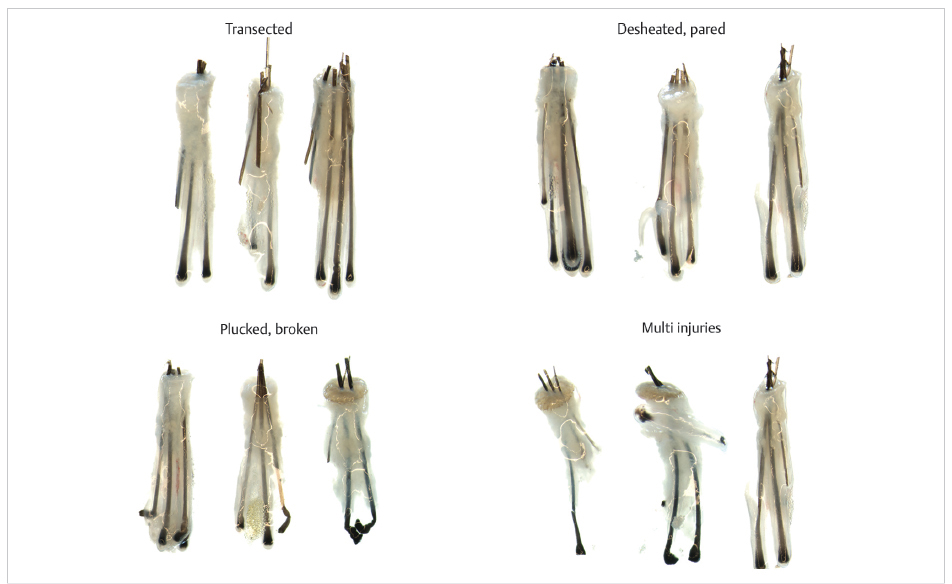
Fig. 60.2 Different kinds of graft injuries.
The grafts should be examined under the microscopes to evaluate overall quality. FUE grafts tend to be skinny especially if they are extracted using a small-diameter punch and if the dissection is not deep. It is possible that this lack of tissue around the hair has a negative impact on regrowth.
Just as Seager before him, Beehner (1999) showed that FUT grafts are less likely to grow if they contain less protective tissue around the follicles.3 It is likely that FUE transplants are more vulnerable due to the fact that they have relatively lower amounts of tissue surrounding the follicle. Personally, the author believes newer punch designs that have flat or blunt anterior surface or more flared outside cutting edges allow deeper dissection and more tissue to remain on the FUE grafts (Fig. 60.3). The author is also not in favor of using a punch less than 0.8 mm, which by virtue of their small size produce very thin grafts.

Fig. 60.3 Different kinds of grafts: skinny, chubby, and fatty.
Experience has shown that it is not necessary to count and calculate an overabundance of factors to get a good estimation of the quality of the extraction. The Excel program the author uses calculates four fundamental values. For each surgery, the author makes the following calculations:
•Rate of missing graft (MGR): Should be less than 5% (punch attempts–the number of grafts yielded).
•Calculated follicles per graft expected (CFGE): Hairs/graft expected transection of 0%.
•Calculated follicles per graft achieved (CFGA): Actual number of hairs/graft obtained.
•The difference between CFGE and CFGA: Indication of the follicle transected rate (FTR).
Chapter 52b (Follicular Unit Excision Terminology) discusses the definition of these values in more detail.1,2
Table 60.1 demonstrates the use of these key values in an FUE procedure to compare graft quality using two different punch sizes.
Table 60.2 Punch comparison using key values
Hybrid trumpet punch diameter | 0.85 mm | 0.9 mm |
Attempts | 100 | 100 |
Grafts obtained | 97 | 98 |
MGR | 3% | 2% |
CFGE | 2.31 | 2.35 |
CFGA | 2.15 | 2.25 |
Difference CFGE, CFGA | 0.16 | 0.10 |
FTR | 6.9% | 4.3% |
Abbreviations: CFGA, calculated follicles per graft achieved; CFGE, calculated follicles per graft expected; FTR, follicle transected rate; MGR, rate of missing graft. | ||
One big advantage of using CFGE and CFGA is that it gives the most precise estimate.
Having an FTR of 5% with a 1-mm punch diameter and a CFGE of 2 does not yield the same graft quality as a 0.8-mm punch diameter with a CFGE of 2.3 as we must also compare CFGA with the calculated density of the donor area.
In general, the author leans toward the use of a sufficiently small punch, with a diameter between 0.8 and 1 mm (the author most frequently uses a 0.9-mm punch). The author would rather get grafts relatively richer in follicles for an average donor area. However, when the area is depleted, sometimes you should opt for an average follicle count (CFGA) of less than 2. The author always tries to have less than 5% transection and less than 10% FTR—the ideal FTR being around 5% (Table 60.2).
Table 60.3 Relationship between punch size and various factors
No. of possible punch insertions | Hairs/grafts | Transections | Scar size | |
Small punch between 0.7 and 0.85 mm | +++++ | +++ | +++ | + |
Medium punch between 0.9 and 1.05 mm | +++ | ++++ | ++ | ++ |
Large punch between 1.1 and 1.25 mm | ++ | +++++ | + | +++ |
In the field of hair transplantation, erroneous assumptions are frequently made that a certain technique or apparatus is capable of achieving ridiculously low transection rates between 1 and 3%. According to the author’s personal experience, in reality these figures are the exception rather than the rule and should, under no circumstances, be considered the norm. Actual rates of transection are rarely calculated to a sufficient degree of accuracy and are most often simply estimates.
An interesting point to keep in mind is that when we compiled the terminology developed by John Cole, Bob True, Jose Lorenzo, and Jean Devroye,1,2 we decided to calculate the transection rates by the number of grafts effectively extracted and not the total number of attempts. This means that a complete transection, if not harvested and placed with the other grafts in the grafts to be counted, will be considered a missing graft and will not be included in the calculation of the transection rate. Buried grafts, which have very little chance of regrowth and which will likely produce a cyst, are also considered missing grafts. The MGR is therefore as important as the rate of transection. It is unfortunate that very few practitioners are measuring the rate of missing grafts, which is essential to an accurate calculation of transection rates.
Another important measure is the number of damaged follicles. There are no studies yet on the impact of these injuries on regrowth, but it is likely that this has real consequences on the regrowth and/or final diameter of the hair observed.
The following types of damage should be avoided as much as possible during the extraction process: paring2 and fractures of the dermal papilla (DP) and hair bulb.2,4 To date, no study has been carried out to find out how these injuries influence regrowth. On the other hand, there was a study that consisted of transplanting all of the rejected FUT grafts that were usually thrown away and regrowth was observed in a certain portion of those grafts.
Extraction Phase (Removing Grafts after Excision)
This intermediate phase is often neglected, left to the discretion of the assistants and too quickly executed or without enough care and experience, which can result in severe damage. Success in this phase requires an ideal balance of traction on the graft and pressure on the skin.
Excessive pressure on the bulge should be avoided in order to avoid trauma to the graft. The author is an enthusiast of blunt punch dissection because in general he can always dissect to a depth of 4 mm. This depth allows for a more complete separation of the follicular group from the surrounding skin and the implication is that less force is required to remove the graft from the skin. The author thinks that excessive force applied to the follicles, especially when applied at the bulge region, can lead to follicle damage and poor growth. Serrated forceps should always be used as they hold the graft securely without compression, and grasping multiple areas of the graft (hand over hand) to distribute the force along the length of the follicles is a reasonable strategy to prevent crush injury. Choosing high-quality instruments is essential to avoiding damage during extraction. The author uses the serrated diamond forceps sold by Robbins Instruments USA. Placing two pairs of forceps along the length of the follicle distributes the force over a longer length and minimizes trauma to the graft.
The Cole Instruments Aide to Extraction (ATOE) device is another instrument that can be used. It was developed to extract multiple grafts successively and keep them on the clamp without causing damage.
Good hand–eye coordination and gentle pulling in the correct direction are required to manually extract the grafts gently. There are many subtle differences in the pulling technique; the standard of care in hair restoration allows hair technicians to remove the graft. However, physicians should be skilled in this task and be able to monitor their technician’s performance.
The depth of penetration must be adequate to cut through the attached structures—arrector pili muscle and sebaceous gland, and beyond the bulge region of the follicle. If the follicle is released properly from the attached dermal structures, the previously scored graft should be easier to extract.
If the graft is not adequately released due to an inadequate penetration depth or stronger attachments, higher extraction forces are required to remove and separate the graft from the attached dermal tissues. This may lead to a higher incidence of “capping” of the epidermis–dermal tissues. The author recommends leaving this graft in place as the epidermis will regrow. This graft is counted as a missing graft (Fig. 60.4).
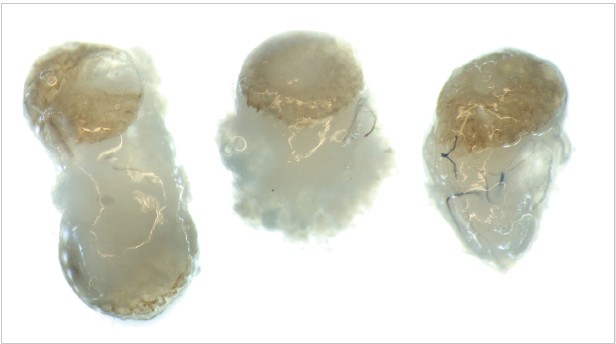
Fig. 60.4 Capping.
Related posts:
 Hair Anatomy and Histology for the Hair Transplant Surgeon
Hair Anatomy and Histology for the Hair Transplant Surgeon
 Plugged in: How to Ensure That Your Practice Thrives (and Survives) in Today’s DigitalWorld
Plugged in: How to Ensure That Your Practice Thrives (and Survives) in Today’s DigitalWorld
 Transplanting into Areas of Cicatricial Alopecia
Transplanting into Areas of Cicatricial Alopecia
 Special Considerations for Postoperative Care in Follicular Unit Excision
Special Considerations for Postoperative Care in Follicular Unit Excision
 Hairline and Recipient Area Repair of Poor Previous Transplantation
Hairline and Recipient Area Repair of Poor Previous Transplantation
 Ergonomics in Hair Restoration Surgery: FUE Technique
Ergonomics in Hair Restoration Surgery: FUE Technique
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


