Propeller flaps represent an outstanding alternative to conventional pedicled and free flap options in lower extremity reconstruction, offering significant advantages over the latter. An understanding of the perforasome concept, hot and cold perforator locations, and basic flap design enable the surgeon to readily harvest flaps based on any clinically relevant perforator in freestyle fashion. The purpose of this article is to review fundamentals of propeller flap design and harvest in the lower extremity and discuss reconstructive strategies by level of injury.
Key points
- •
The propeller flap is a workhorse pedicled perforator flap designed as an island flap that reaches the recipient site through an axial rotation.
- •
Advantages to propeller flaps include minimal donor site morbidity, preserving axial blood supply to the distal extremity, excellent tissue quality match, and significantly less physiologic demands on the comorbid patient.
- •
Literature-reported complication rates in propeller flap reconstruction of the lower extremity compare similarly to free tissue transfer.
- •
An understanding of the perforasome concept, hot and cold perforator locations, and basic propeller flap design will enable the surgeon to readily harvest flaps based on any clinically relevant perforator in freestyle fashion; however, each level of injury has preferable perforator source options.
Introduction
The advent of perforator flaps has ushered in a new and exciting era for reconstructive surgery. Although not a panacea for the lower extremity, pedicled perforator flaps (PPFs), and propeller flaps in particular, have seen increased application, replacing traditional locoregional options and free tissue transfer in the appropriate settings. Most commonly, their indication includes small- to medium-sized defects of the distal third of the leg, a challenging predicament given limited local donor tissue availability; they do have utility in smaller defects of other areas of the leg also. The propeller flap is a workhorse subset of PPFs, defined as a completely islanded flap that reaches the recipient site through an axial rotation.
Propeller flaps carry significant advantages, including minimizing donor site morbidity and pain, sparing the underlying muscle, preserving axial blood supply distally, and providing excellent tissue match. Compared with free flaps, propeller flaps obviate the requirement for microsurgery and position changes; additionally, they are less morbid for unhealthy patients, and reduce operative and hospitalization time and costs.
This article discusses the principles of PPFs, propeller flap design, and considerations by location along the lower extremity.
Perforator flap anatomy
Understanding perforasome theory is key to propeller flap success. Areas of high perforator density are termed hot spots, while those of a relative paucity are cold spots. In the extremities, hot spots are located adjacent to articulations and at midpoints between 2 articulations; in the trunk, hot spots are parallel to the anterior and posterior midline and the midaxillary line. , ,
Perforators communicate bidirectionally with one another in series through direct (suprafascial) and indirect (subdermal plexus) linking vessels. With adequate filling pressures through 1 perforator, there is interperforator flow to the adjacent perforasome(s), thus explaining how large flaps can be based off of single perforators. Linking vessels are oriented longitudinally in the extremities and perpendicular to midline in the trunk. Furthermore, extremity interperforator flow tends to occur away from articulations versus multidirectional for midpoint perforators. Flow also generally perfuses same-source artery perforators before other-source perforators. These principles form the basis for flap design, whereby flap length and skin paddle orientation should be based on the orientation of the linking vessels (ie, axially in the lower extremity).
The angle of perfusion is another element to consider. When perforators are located at the most proximal aspect of the flap (eccentric), geometric design of the proximal skin paddle (superior angle of the tissue edge proximal to the perforator) influences distal perfusion. Specifically, as the angle increases, more linking vessels are captured, thereby augmenting distal flap perfusion through enhanced interperforator flow, and vice versa. The influence of interperforator flow by the angle of perfusion is less impacted with centrally located perforators, as a more centrally based pedicle captures more linking vessels.
Indications and contraindications
The perioperative considerations in propeller flap reconstruction of the lower extremity are nearly identical to more traditional approaches and include timing, comorbidities such as vascular disease, and nutrition, radiation, trauma mechanism, and nicotine use. Comorbidities such as diabetes and peripheral vascular disease are posited to increase flap necrosis. Ultimately, although healthier patients are more ideal candidates, those with multiple comorbidities benefit from avoiding a large, complex free flap reconstruction.
In the trauma setting, the injury should be allowed to fully declare and radical debridement achieved, with early reconstruction being generally preferred. The temptation to sacrifice extent of debridement to limit defect size should be avoided.
In the oncologic setting, one should consider delaying reconstruction until pathology indicates clear margins. Additionally, although propeller flaps provide durable coverage that can withstand radiotherapy, previously irradiated wounds mostly require new, well-vascularized tissue via free flap.
The principle indication for propeller flaps includes small- to medium-sized defects with exposed critical structures for which alternatives like skin grafting are inadequate. Size limitations for safe flap design are not firmly understood. Authors have suggested limitations based on clinical experience, while cadaver-based studies have sought to define perforasome areas. In a 2012 systematic review, mean leg defect size reconstructed with propeller flaps was 37.4 cm 2 , ranging from 4 cm 2 to 180 cm 2 .
Preoperative evaluation and special considerations
Preoperative imaging is not routinely mandated, as flap dissection can be conducted in freestyle fashion. Nonetheless, Doppler evaluation is quick and prudent. Computed tomography (CT) angiography and other advanced modalities can be obtained as needed, such as investigating vascular integrity after trauma or backup options including free tissue transfer. Other adjuncts like smartphone-based thermography and color duplex have also been employed. ,
The lower extremity represents 46% of the adult total body surface area, with a mean of 93 plus or minus 26 perforators in each extremity. Each clinically relevant perforator can theoretically be incorporated into freestyle flap design; thus flap options are virtually limitless. Here workhorse options are briefly reviewed by level including clinical examples ( Table 1 ).
| Location: | Traditional Flap | Propeller Flap |
|---|---|---|
| Groin | Sartorius, TFL, RAM | SFA |
| Thigh | Leg muscles, RAM, free flap | Rarely indicated; SFA, LSGA |
| Peripatellar/popliteal fossa | Gastrocnemius, thigh muscles | MSA, SFA/DGA, LSGA, MSFA, |
| Upper third leg | Gastrocnemius | MSA, PA, PTA, ATA |
| Middle third leg | Soleus | MSA, PA, PTA, ATA |
| Distal third leg/ankle | Free flap, reverse sural flap | PA, PTA, ATA |
Superficial Femoral Artery Perforator
The medial thigh yields numerous flaps of varying and inconsistent nomenclature based on the superficial femoral artery (SFA), medial circumflex femoral artery, and lateral circumflex femoral artery. , SFA flaps are reliably harvested from a mean of 5 perforators, roughly half musculocutaneous, for coverage ranging from the groin, distal thigh, knee, and even proximal tibia and posterior calf. Miyamoto and colleagues reconstructed groin defects with flap sizes up to 19 × 8 cm eccentrically oriented along the axis of the sartorius (approximating the SFA).
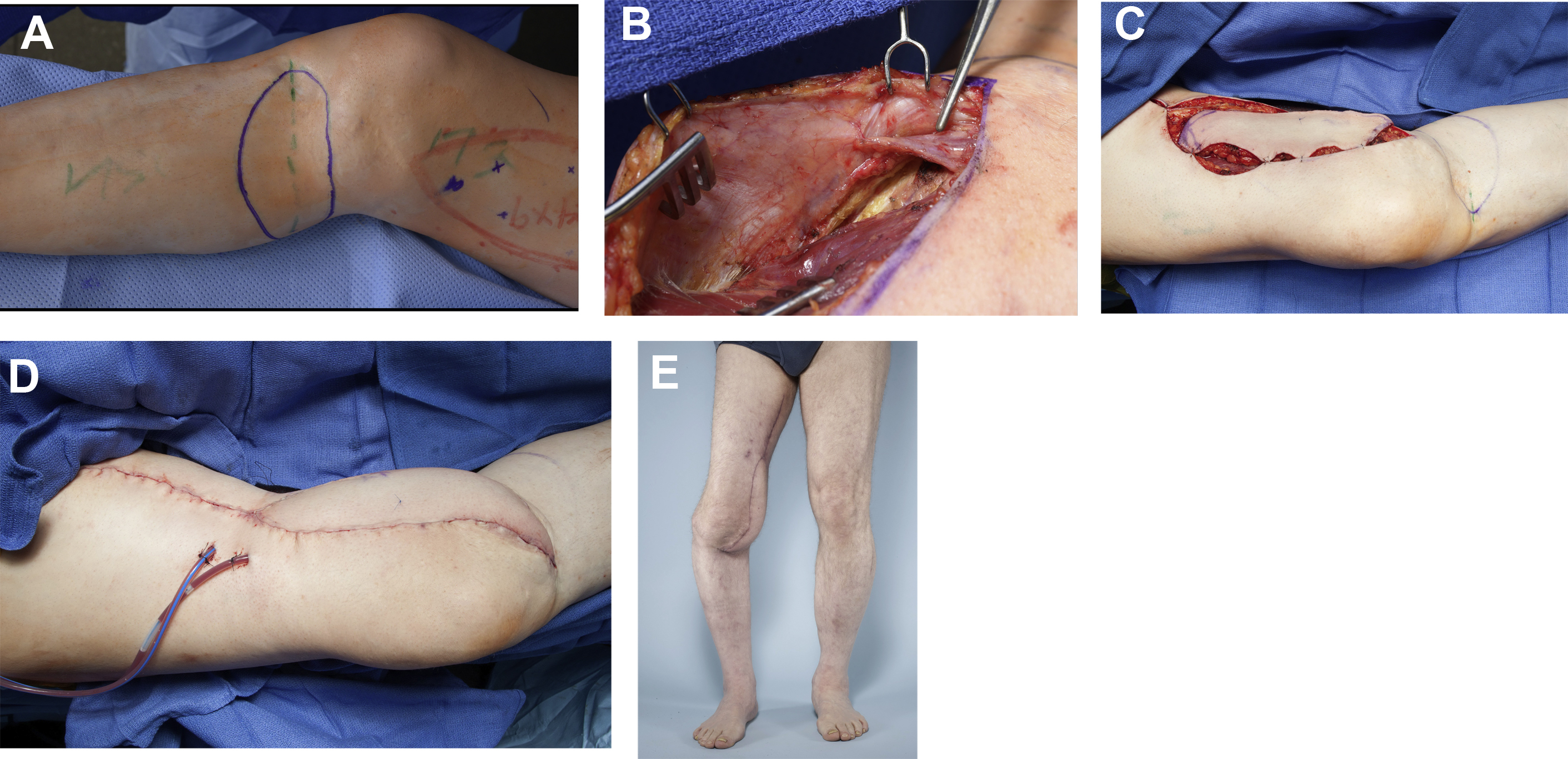
In the distal thigh, perforators from the SFA (62%) and its principle distal branches, the descending genicular (15%) and saphenous (23%) arteries, can support critical coverage of the knee and popliteal fossa ( Fig. 1 A–E, Case 1 below). , ,
Lateral Supragenicular Artery Perforator
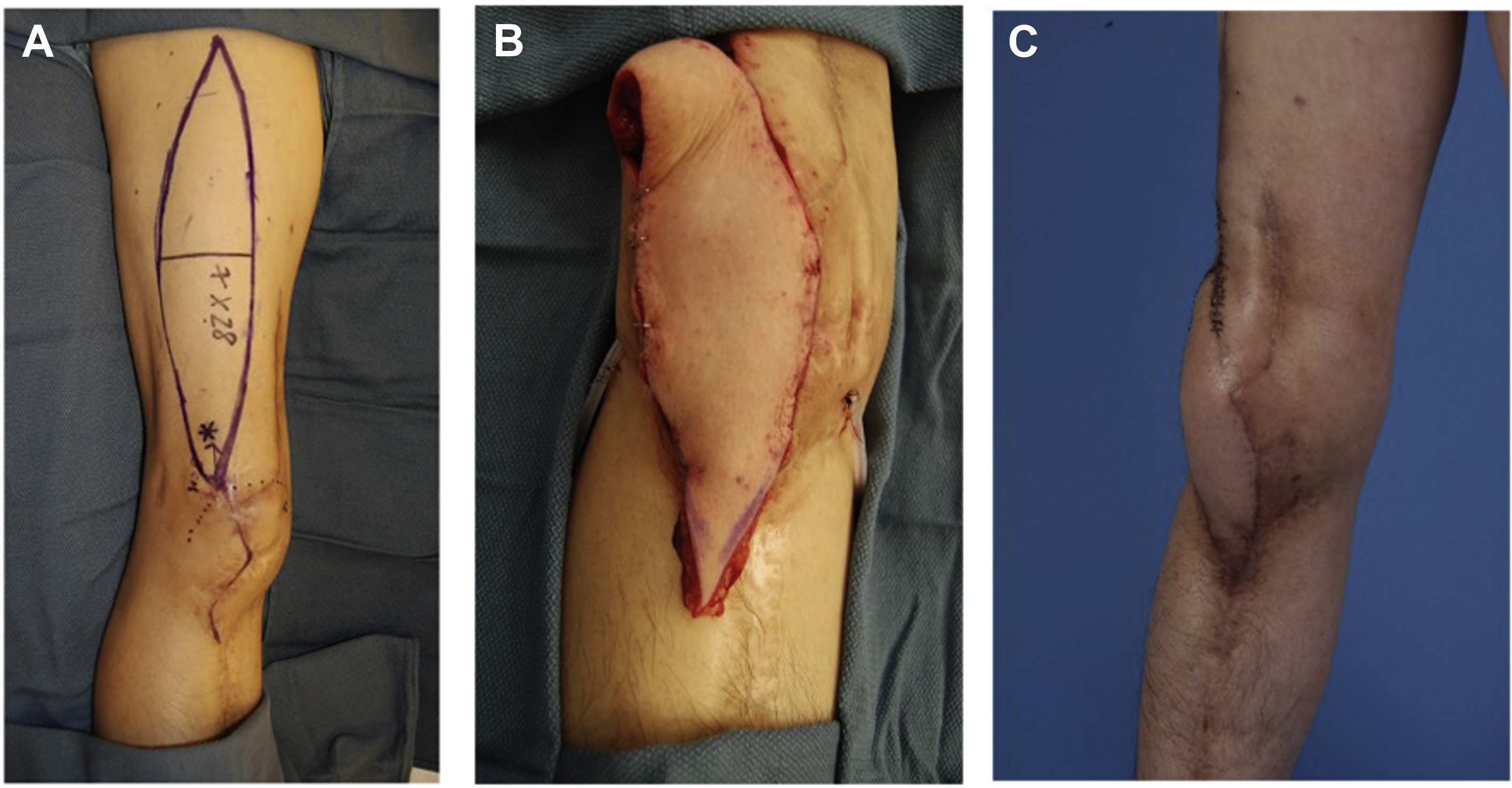
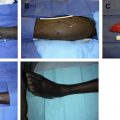
The lateral supragenicular artery (LSGA) perforator flap represents another workhorse alternative to the gastrocnemius for locoregional coverage of the knee and popliteal fossa ( Fig. 2 A–C, Case 2) . Two perforators are localized within 5 cm laterally and 7 cm proximally from the superolateral patella, and the flap is designed eccentrically from the perforator up to the mid-thigh. Compared with the distally based ALT flap, the LSGA perforator is closer in proximity to the knee and does not as easily suffer venous congestion. The senior author has designed flaps up to 270 cm 2 for knee coverage.
Lower leg
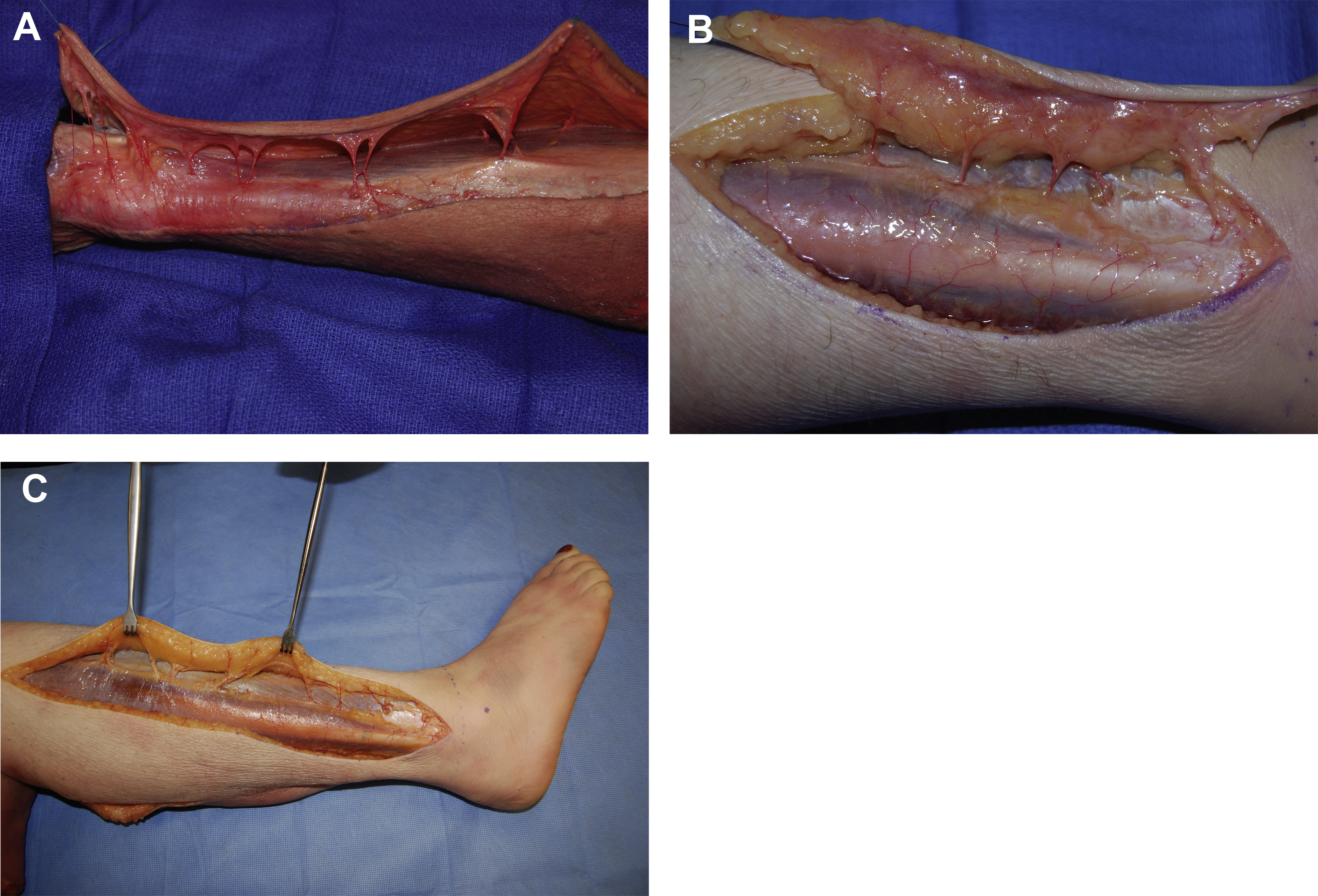
Both musculocutaneous and septocutaneous perforators pierce the crural fascia in 4 longitudinal rows (1 row for each major source artery) along the intermuscular septa bordering the compartments of the leg ( Fig. 3 A–C).
Related posts:
 Freestyle Local Island Pedicle Flap in Lower Leg Reconstruction
Freestyle Local Island Pedicle Flap in Lower Leg Reconstruction
 Free-Style Free Perforator Flaps in Lower Extremity Reconstruction
Free-Style Free Perforator Flaps in Lower Extremity Reconstruction
 Free Flaps in Lower Extremity Reconstruction
Free Flaps in Lower Extremity Reconstruction
 Orthoplastic Approach to Lower Extremity Reconstruction
Orthoplastic Approach to Lower Extremity Reconstruction
 The Anterolateral Thigh Perforator Flap
The Anterolateral Thigh Perforator Flap
 Lower Extremity Reconstruction in the Pediatric Population
Lower Extremity Reconstruction in the Pediatric Population
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


