CHAPTER 27 Primary and Secondary Mastopexy-Augmentation
Summary/Key Points
Introduction
The idea of treating hypoplastic and ptotic breasts with a combined implant and lift was first described in the 1960s by Gonzalez-Ulloa and Regnault.1,2 Since then, there has been much written on the subject, both in support of the procedure and in cautioning about the potential risks and possible adverse outcomes.
Cardenas-Camarena published his experience with 384 patients undergoing one stage mastopexy-augmentation.3 His complication rate of 18%, all described as minor, was very favorable. His approach was to first insert the implant and then plan the skin excision around the newly implanted breast. He provided guidelines for the pattern of skin excision based primarily on the degree of ptosis of the nipple–areola complex (NAC) and on the distance from the NAC to the inframammary fold (IMF).
In 2007 Stevens reported on 321 consecutive one stage mastopexy-augmentations.4 Approximately two-thirds of these were primary procedures and one-third were in patients with previous breast augmentation or previous breast lifts. Complications over an average 40 month follow up were rare and included saline implant deflation, poor scarring, recurrent ptosis and areola asymmetry. The total revision rate was 14.6% with three-quarters of these being implant related and one-quarter being tissue related. He compared these results favorably to a 13% revision rate in his breast implant only patients and an 8.6% revision rate in his mastopexy only patients. Stevens noted that revision was most common in smokers, those undergoing a circumareolar lift and patients having augmentation with saline implants. He concluded with the statement that ‘although a revision rate of 14.6% is significant, it is far from the 100% reoperation rate required for a staged procedure.’4
Spear has written about his experience with combined breast augmentation and breast lift and cautions about the increased risks and revisions associated with this approach.5 He noted a 10-fold increase in complications when comparing primary augmentation mastopexy with primary augmentation only. As a guideline, he recommended that women undergoing breast augmentation could avoid a simultaneous mastopexy if the nipple sits at or above the IMF, if the nipple and areola are visible on the front of the breast with some inferior non-areola skin being visible, if the breast overhangs the IMF by no more than 2 cm and if the nipple to IMF distance is less than or equal to 8 cm under maximum stretch.
It is important to differentiate between primary one stage augmentation mastopexy and secondary procedures that are performed following a previous implant or lift. Handel’s paper titled ‘Secondary mastopexy in the augmented patient: a recipe for disaster’,6 highlights some of the key issues that must be considered in this complex patient population. Over time, augmented breasts, especially those placed in a subglandular plane, become ptotic and develop thinning of the overlying breast tissue. The majority of these soft tissue effects are seen in the lower pole of the breast. Often, there are associated contractures of the surrounding capsules. Correction of this deformity may require explantation only, mastopexy with explantation or mastopexy with or without implant exchange or pocket change7 (Figs 27.1 and 27.2).




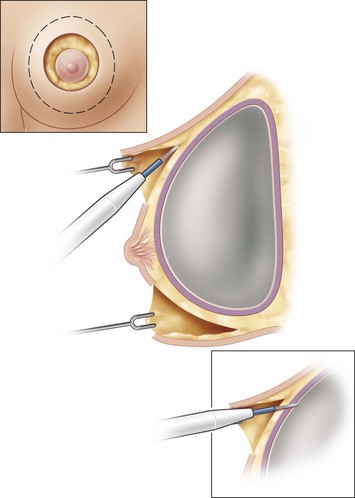
Handel makes several recommendations for dealing with these patients. Preoperative deflation of a saline implant allows the patient to see the breast in a deflated state and allows the surgeon to better assess the quality and quantity of remaining breast tissue. This simple step will provide valuable information that may affect the choice of operation selected by the patient. If a mastopexy is required, undermining should be minimized and capsulectomy should only be performed when necessary. It is important to make note of previous breast scars, especially as they relate to the vascular supply of the NAC. Since inferior pole tissues are often attenuated, use caution in selecting an inferior based pedicle. It may often be best to excise the thin lower pole tissues and select a superiorly based pedicle, where tissues are of better quality. Finally, in circumareolar incisions, especially with a subglandular implant, it is important to bevel the plane of dissection acutely due to the thin nature of the tissue between the skin and the underlying implant. Failure to recognize this may lead to vascular compromise of the nipple (Fig. 27.3).
Patient Selection
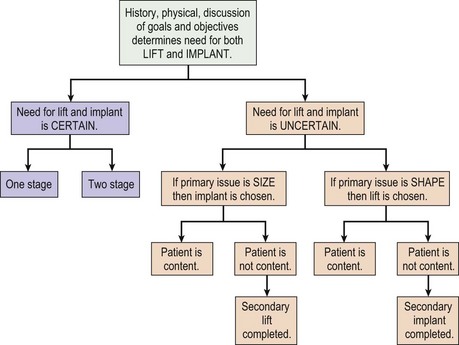
The fundamental decision that must be made between patient and surgeon is what is the best operation to most closely meet the patient’s goals and objectives of surgery. This may be a mastopexy, an augmentation or a combination of both. Although some patients can only be adequately treated with a combined procedure, every consideration should be made to addressing the patient’s concerns with a single procedure, if possible (Figs 27.4 and 27.5). Initially, the patient’s goals must be clearly reviewed. Are the concerns related to size, shape, symmetry, NAC position, areola size, stretch marks or some combination? Which of these is most important to correct and what is the patient prepared to trade off in order to obtain this correction? Essentially, a risk benefit analysis must be applied after a thorough discussion about options and complications. If a mastopexy and augmentation are to be performed together, a further decision of whether or not to perform the surgery in one stage or two stages is necessary. A one-stage approach should be reserved for healthy patients, non-smokers with few risk factors for impaired healing. These patients should be certain that they desire both a lift and an implant, otherwise the issue most important to the patient is treated first. Once healed, the patient can determine if they require the second procedure to satisfy their goals. A decision tree can be helpful in performing this analysis (Fig. 27.6).
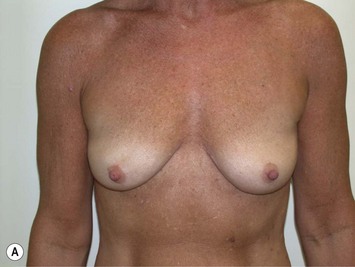







Fig. 27.5 A, B Preoperative views of patient with ptosis and good breast volume. C, D Six week postoperative views following vertical scar mastopexy using an inferior flap secured under a pectoralis sling.9
Physical examination focuses on overall body proportions and the relationship of breast size to the rest of the body. Breasts are examined for size, shape, symmetry, nipple position and stretch marks. Ptosis is assessed as defined by Regnault.8 It is important to assess the quality of the breast tissue and skin in all zones of the breast. This information is helpful in deciding whether tissue should be excised and if so, then from which zone. Standard measurements of sternal notch to nipple, nipple to IMF, breast width and nipple to midline are documented. Finally, a breast examination is performed for abnormal masses.
Indications
Operative Technique (Table 27.1)
Markings
Table 27.1 Summary of operative steps for primary mastopexy-augmentation
Once the height of the NAC is determined, the remainder of the markings are dependent upon the planned skin pattern of excision. Whether marking out a crescent lift, a circumareolar excision, a vertical skin pattern or a Wise pattern excision, markings should be very conservative with the expectation that more skin will be excised at the time of tailor tacking (Fig. 27.7).
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


