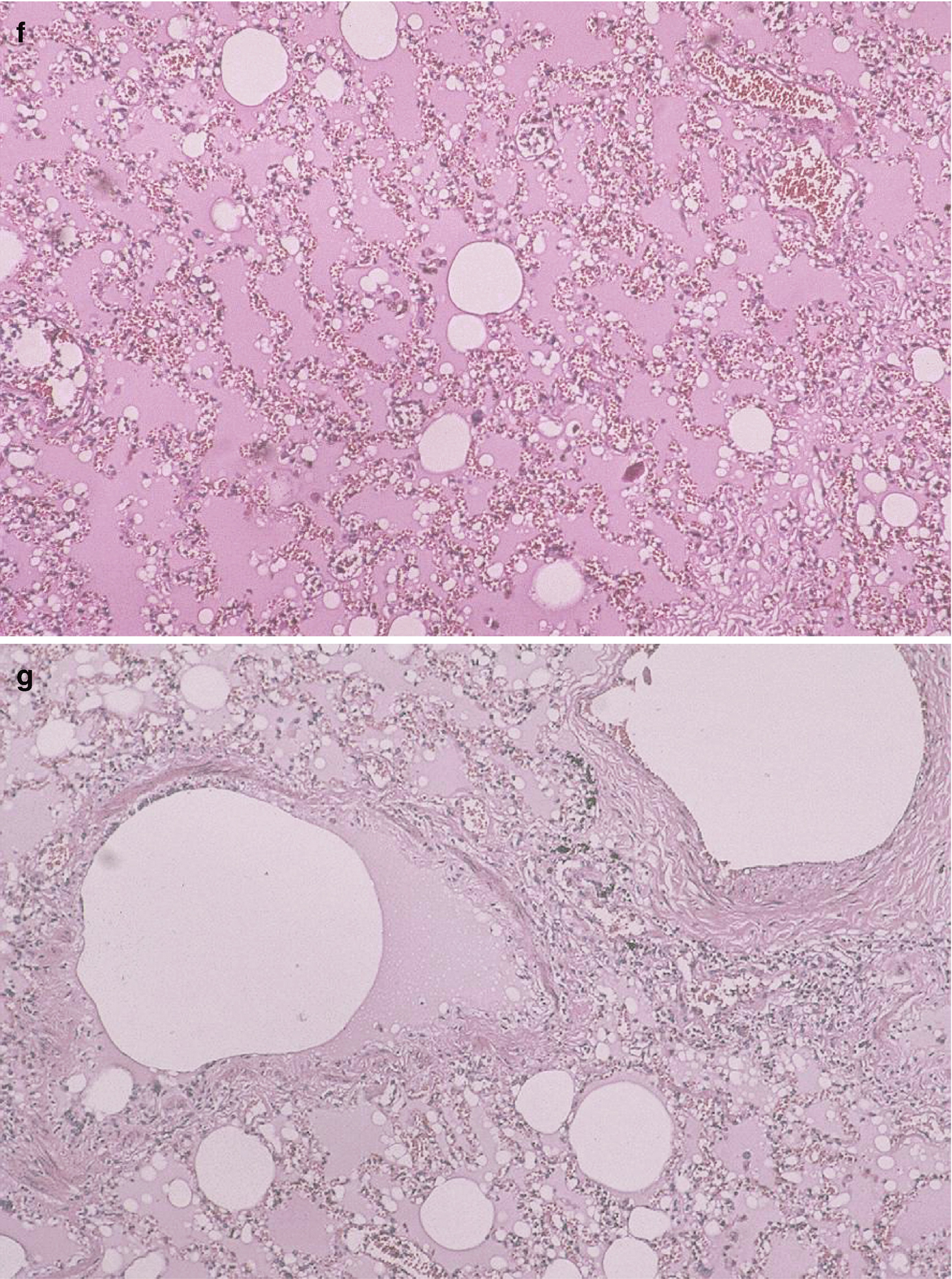
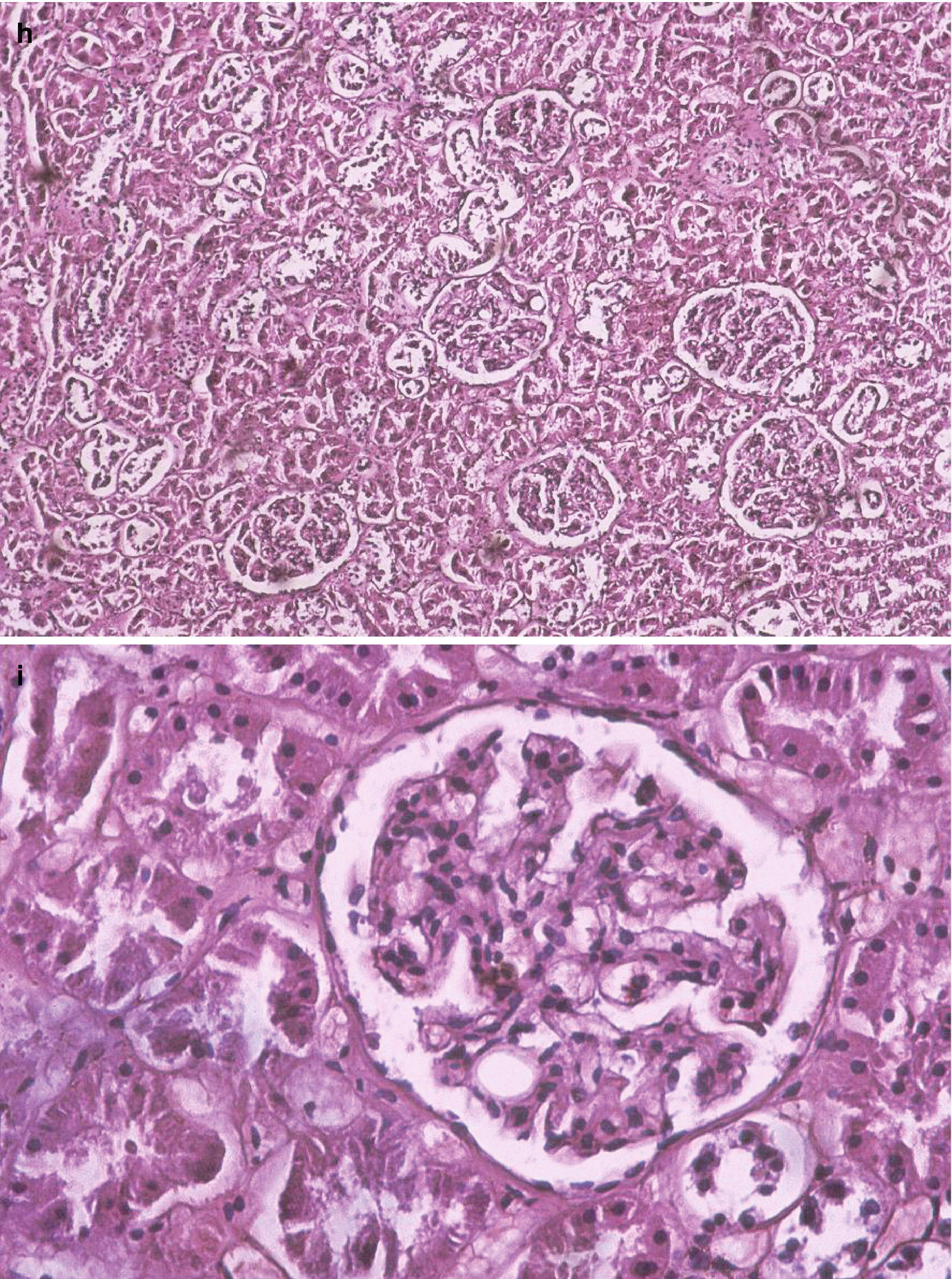
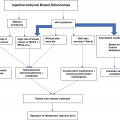
Patient deceased due to pulmonary silicone embolism during the clandestine injection of liquid silicone into her breasts. (a) Side view on the Morgagni table. (b) Front view. (c) Left breast with a puncture wound in the inferior-internal quadrant. (d) Left breast with a puncture wound in the super-external quadrant. Note the home-made bra used immediately post-injection, placed to seal the silicone in its desired location. (e) Pool of intramammary silicone found during autopsy. (f) Lung micrograph, hematoxylin-eosin stained, 10× magnification. Thrombosis of blood vessels, marked hyperemia, intra-alveolar edema, and clear vacuoles without dye affinity in the arteries and capillaries are observed. (g) Same as in (f) but at 40× magnification. (h) Kidney micrograph, hematoxylin-eosin stained at 10× magnification. Glomerular capillaries are observed with clear globules but no dye affinity. (i) Same as in (h) but with 40× magnification. (Photos: courtesy of Dr. J. Herbstein)
In the dermis, two puncture-type wounds 0.3 cm in diameter were observed, one located in the upper outer quadrant of each breast (Fig. 5.1c, d) [1], the right one larger than the left. When the area around it was compressed, a substance with an oily, transparent appearance and consistency emerged from each wound.
A sample of this transparent, oily substance, from the left breast, was sent to the chemistry laboratory for identification.
A histopathological study of the subcutaneous and muscular cell tissue of the pectoral region, as well as brain, cardiac, pulmonary, hepatic, and renal tissue was requested. The paraffin inclusion and hematoxylin-eosin staining technique yielded the following results.
The brain had areas of demyelination, edema, and perivascular hemorrhage. Both lungs exhibited blood vessel thrombosis, accentuated hyperemia, intra-alveolar edema, and clear vacuoles without dye affinity for hematoxylin-eosin in either arteries or capillaries (Fig. 5.1f, g) [1]. Sinusoidal spaces of the liver were congested, with fatty degeneration in the periphery of the central vein. The heart had preserved histological architecture. A fragment of fatty tissue that covered the muscular tissue extracted from the pectoral region exhibited cystic areas with gelatinous content and areas with clear vacuole infiltrates, but no dye affinity for hematoxylin-eosin. The kidney had glomerular capillaries, with clear globules and no dye affinity for hematoxylin-eosin (Fig. 5.1h) [1]. The changes described here indicate the presence of multiple fat emboli. The chemical laboratory reported that the oily substance sent in for analysis had physical characteristics consistent with silicone.”
The above case illustrates how that injecting silicones for cosmetic purposes may cause pulmonary thromboembolism, which triggered immediate death in the above-described patient. The mechanism behind the pulmonary embolism could be related to the local pressure induced by the injection of large volumes of substance, to the local massage that is frequently associated with this procedure, or to migration or direct injection into vessels. Of these, the last mechanism seems to be what triggered death in the above-presented case.
Certain findings – like hyperemia accentuated by intra-alveolar edema and emboli with clear vacuoles and no tinctorial affinity for hematoxylin-eosin in the lumen of arteries and capillaries – reveal the development of an acute process that, in some patients, triggers death. Another confirmatory element was the discovery of oily material that flowed from the puncture wound when the left breast of the victim was squeezed [sic] [1].
Influenza-Like Syndrome
Some of our patients reported systemic complications after having silicones injected into their breasts, which included a flu-like syndrome characterized by fever; meanwhile, the breasts exhibited edema, tenderness, and generalized cutaneous erythema. These symptoms subsided with the administration of antibiotics and corticosteroids; but when these treatments were discontinued, the symptoms returned with increased virulence.
Other patients whose breasts have been injected with silicones or some other oily substance present with chronic respiratory distress and clinical or subclinical signs of a collagen vascular disease (see Chap. 6).
Case n° 2: Asymptomatic Patient
A girl of 24-year-old, student, consulted our service for hypomastia.
A history was obtained of the injection of 150 cm3 of liquid silicones in each breast 2 years before the consultation. The procedure was performed by a transgender individual in the home.
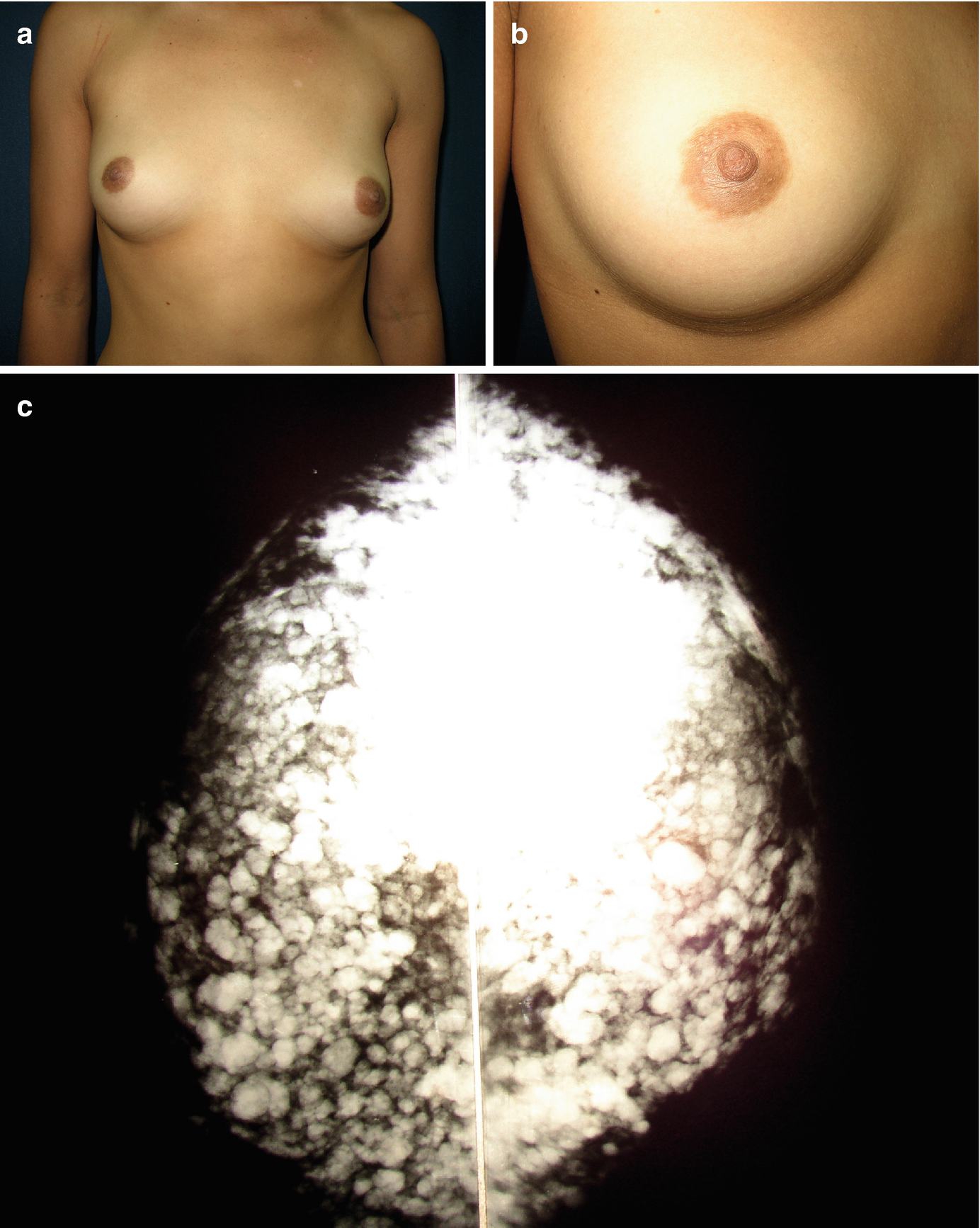
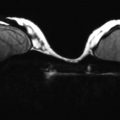
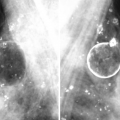
Asymptomatic patient with mammary siliconomas throughout mammary glandular tissue, caused by the injection of liquid silicone. (a) Front view. (b) Close up view. Observe the good aesthetic result obtained with the injection of liquid silicones. (c) Mammography revealed the contrast between the mammographic image, which was totally distorted, and the grossly normal-appearing breasts
Case n° 3: Patient with Cutaneous Erythema
A woman of 40-year-old consulted us for redness of the skin.
On history, prior injection of liquid silicones into both breasts for the purpose of enlargement was verified, having occurred 10 years before the current consultation. This procedure too was performed by a transgender person, in the home.
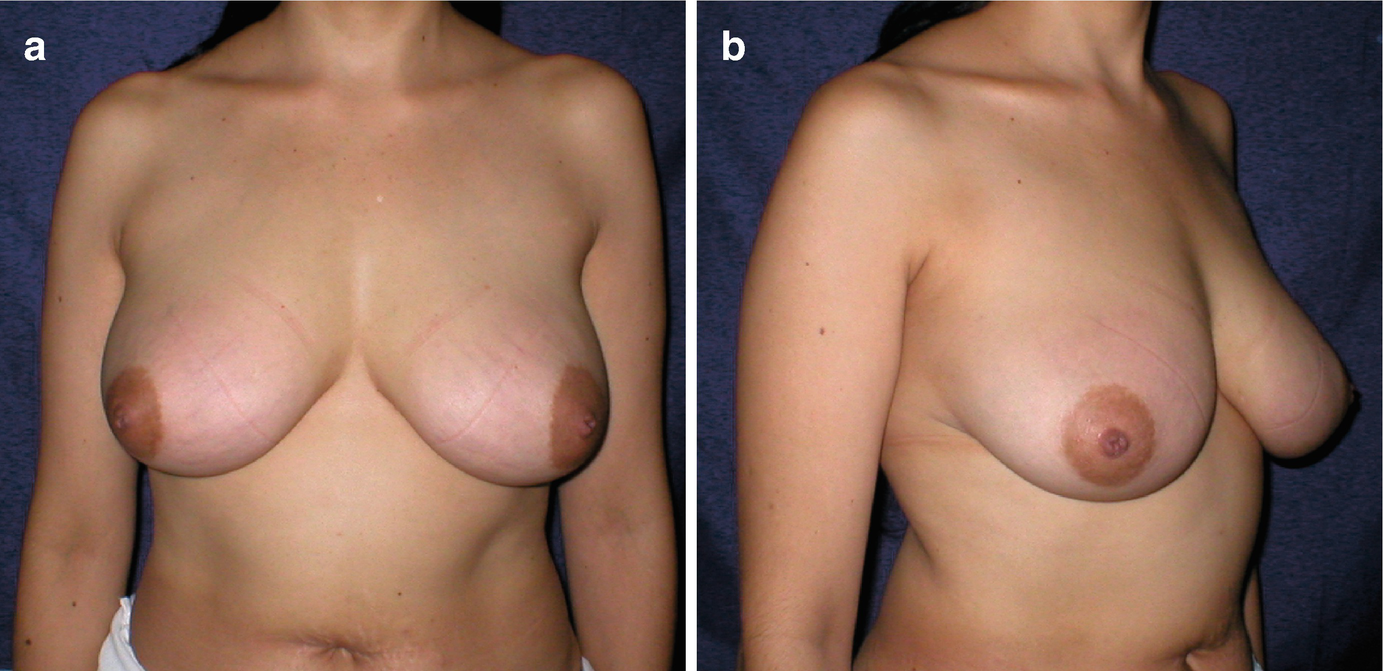
(a) Front view of an asymptomatic patient with mammary siliconomas throughout mammary glandular tissue, caused by the injection of liquid silicone. Observe the mammary erythema. (b) ¾-side view
Case n° 4: Patient with Painful Nodules, But No Cutaneous Involvement
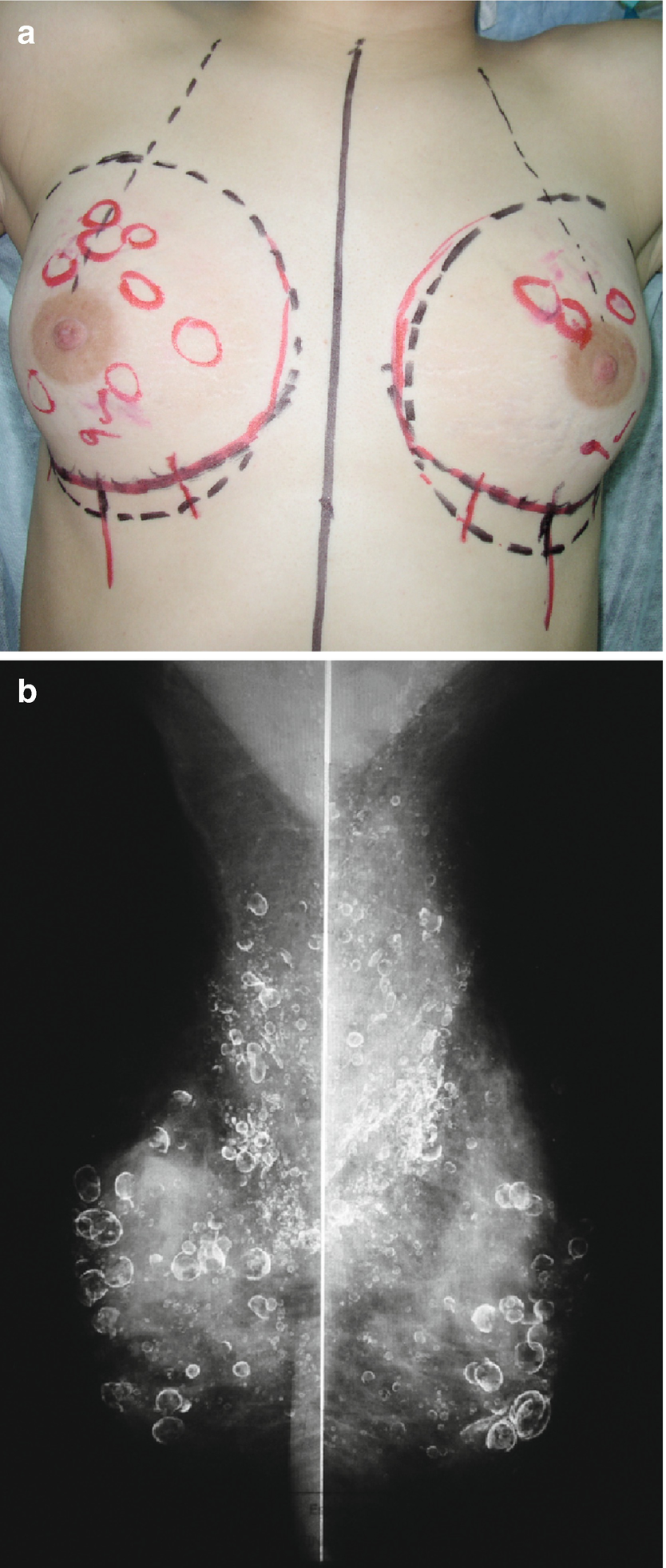
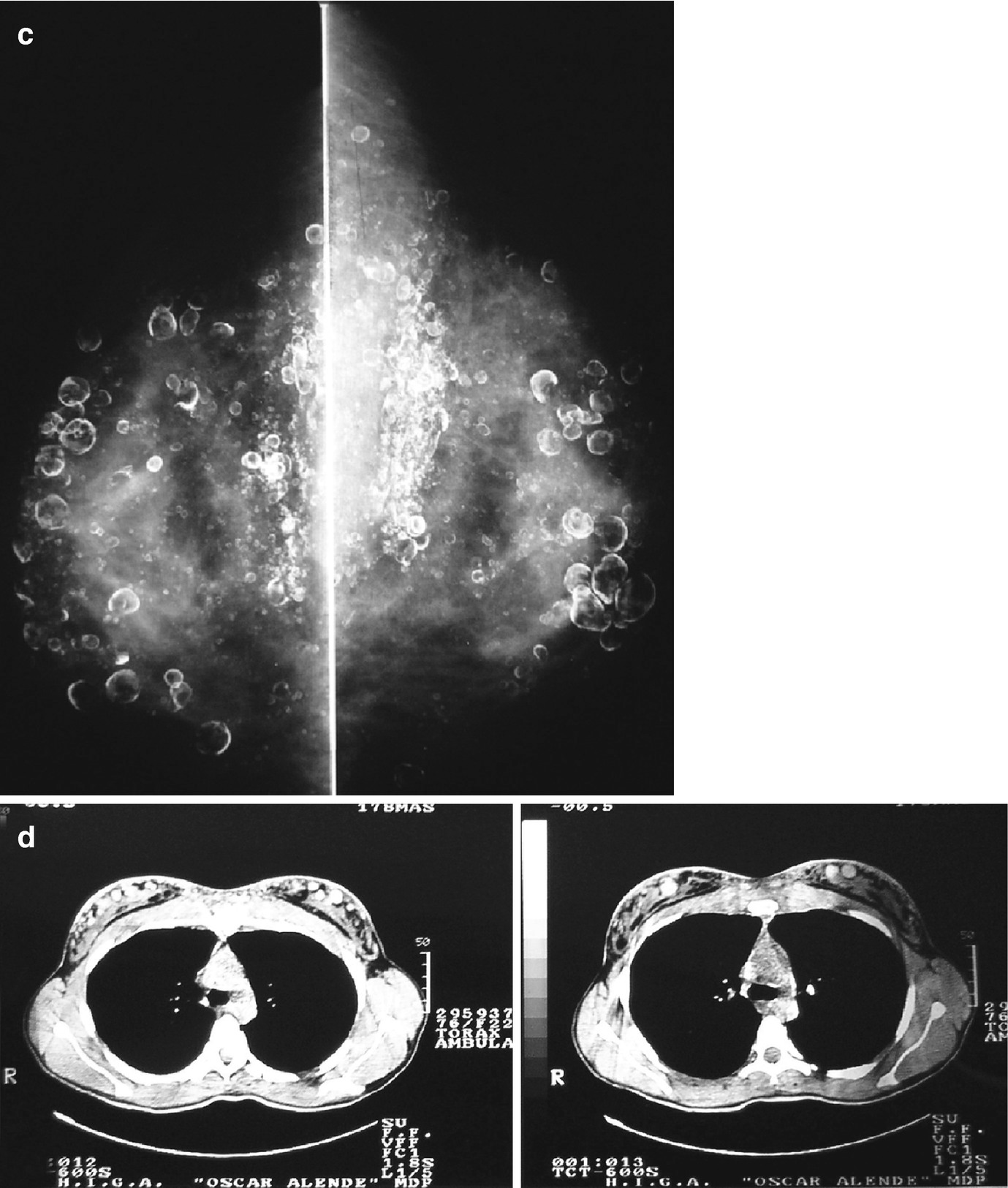
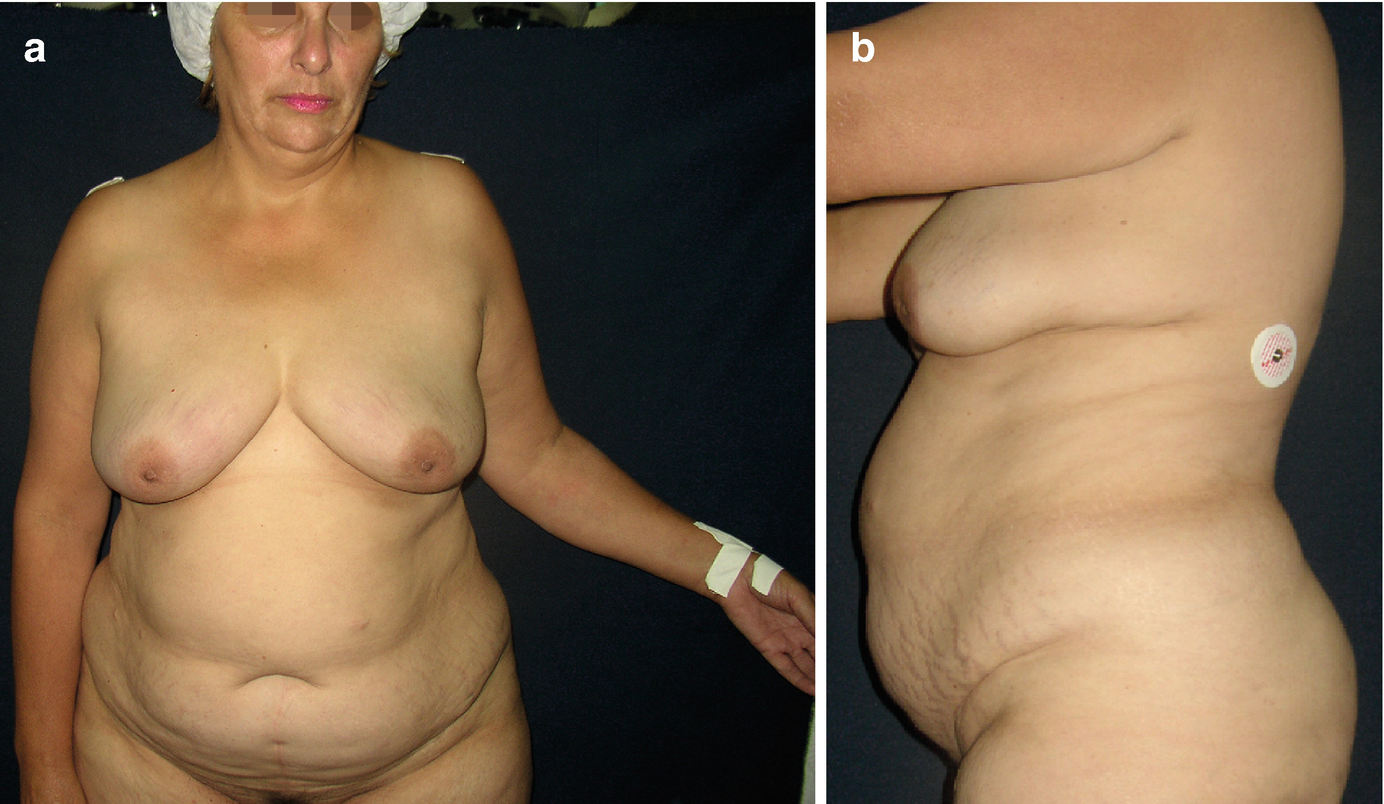
(a) Mammary siliconomas throughout mammary glandular tissue, caused by the injection of liquid silicone. The patient was asymptomatic, and the skin is foldable, not infiltrated by silicones. Note the multiple (painful, palpable) nodules distributed throughout the breast parenchyma. (b, c) Mammography. (d) Multiple siliconomas are identified on MRI
On history, the patient reported that liquid silicone had been injected into both breasts 3 years before the consultation was elicited, the injections performed for the sole purpose of increasing breast size. Again, as with many of these cases, the procedure was performed by a transgender person in the home. The patient reported having been satisfied with the breast shape obtained. However, 2 years after the procedure, palpable tender and painful nodules started to appear, which was the reason for the consultation with us.
On physical examination, a good cosmetic result was verified. However, upon palpation, multiple tender nodules of different sizes were identified, distributed throughout the breast (Fig. 5.4a) [2]. Both mammography (Fig. 5.4b, c) and magnetic resonance imaging (MRI) (Fig. 5.4d) revealed multiple siliconomas distributed throughout the breast parenchyma.
Case n° 5: Patient with Mammary Nodules, But No Cutaneous Involvement

Note the good cosmetic result obtained after the injection of silicones
Case n° 6: Patient with Mild Cutaneous Involvement
A Lady of 56-year-old, professional cook, consulted us for breast skin erythema and multiple painful breast tumors.
Related posts:


Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


