Preoperative Evaluation
Introduction
With the aesthetic concepts outlined in Chapter 1 firmly in mind as a framework, the surgeon can now begin a rigorous preoperative evaluation of a prospective patient. This chapter is divided into two principal sections: preoperative consultation and preoperative analysis. The former reviews in detail the dynamics of an aesthetic consultation as it pertains to fat grafting and/or ancillary methods; the latter undertakes a systematic anatomic analysis of the aging face as it will benefit from fat grafting and/or other techniques.
Fat is not viewed as a universal panacea for the aging face. Instead, this chapter will guide the surgeon in the requisite judgment of when fat will be beneficial and when other rejuvenative techniques may be more applicable. The complementary nature of fat grafting to traditional lifting procedures will be emphasized so that the reader may grasp the role that each type of surgical treatment can play to achieve the optimal aesthetic objective for the patient.
Preoperative Consultation
The goals of an initial preoperative consultation are threefold: (a) to establish what the patient desires as far as aesthetic enhancement, (b) to determine an independent plan based upon a study of the patient’s anatomy, and (c) to ensure that the first two objectives are in alignment. This section will deal chiefly with the patient’s perspective on fat enhancement, that is, understanding what the patient wants and educating him or her about the benefit of fat enhancement versus other ancillary measures. A study of each component of the face has been reserved for the Preoperative Analysis section (even though technically it constitutes part of the consultation).
An aesthetic consultation should always begin with declaration of the patient’s complaint without prodding or prompting from the surgeon. Even if the patient asks for a recommendation, the surgeon should carefully divert the attention back to the patient’s unsolicited expression of desire for enhancement. Listening attentively to the patient’s words will help guide and structure the surgeon’s efforts.
The aging face is a complex and lengthy subject that requires both significant time investment and a commensurate expenditure in thought and energy (for both the surgeon and the patient). Accordingly, starting with what the patient desires can be the most beneficial opening to guide the surgeon in a targeted consultation. If the patient states that
he or she is truly troubled by the deepening nasolabial fold, a conversation about fat enhancement may not be the most fruitful dialogue. Why is this the case? First, we must understand what fat does well and what it does not do so well in our judgment.
he or she is truly troubled by the deepening nasolabial fold, a conversation about fat enhancement may not be the most fruitful dialogue. Why is this the case? First, we must understand what fat does well and what it does not do so well in our judgment.
Fat should be thought of primarily for volume enhancement of the face. It is not an ideal treatment for facial lines or for lip augmentation, although some practitioners have successfully used it in both of these areas. Our experience has been that treating these areas with fat has not resulted in high patient satisfaction. For the treatment of facial lines, fat transfer can oftentimes subject patients to undergo a more significant procedure with more morbidity, and often an inferior result, than if treated with a more standard filling material. Patients who present to the office desiring correction of only hypoplastic lips or deeper facial lines are offered the range of facial filler products tailored to their specific desires, concerns, and budget. An exhaustive review of current filler products lies beyond the scope of this text and will most likely be either outdated by the time of publication or irrelevant for a certain country where a product is unapproved or unavailable.
Although digital imaging analysis with morphing capacity has often been used successfully as an educational tool during a typical consultation, we have not found it valuable for fat transfers. It is difficult to image the projected results of volume augmentation that are normally seen with fat grafting. Alternatively, reviewing before-and-after photographs of patients with similar anatomy and aesthetic complaints can be quite instructive during consultation. It is also helpful to review images of the patient looking at their three-quarter oblique and profile views, as volume changes can best be seen on these views, even though a patient generally only examines himself or herself on frontal view in the mirror. Review of these clinical photographs will enlighten a prospective patient about the effects of volume loss and the benefits of volume restoration. Patients are often surprised by what they learn from these views (Fig. 2-1).
After a detailed preoperative facial analysis (discussed separately in the following section), the surgeon should determine if his or her aesthetic goals match those of the patient. Two other important variables that may affect what procedure(s) a patient selects to undergo are budget and recovery time. The latter consideration can be particularly important when discussing fat transfer, as the time to recovery can be greater than the patient expects due to the relatively noninvasive nature of the procedure. The surgeon should discuss openly and frankly the usual time to recovery after fat transfer and what a “typical” patient looks like during that time. The characteristics of the recovery period are detailed in Chapter 4.
Preoperative Analysis
For simplicity, the face is partitioned into three main components––the upper face, the midface, and the lower face––each of which are subdivided into smaller anatomic subunits. The analysis in each anatomic zone pays attention to whether fat alone, an alternative technique, or a combination approach is preferable. This section will help the reader to determine which methods will be the most suitable to achieve the ideal aesthetic principles outlined in Chapter 1 (Fig. 2-2).
Upper Face
Brow
The upper face is an important area concerning the transformation of a patient from looking tired to looking more awake and vibrant. However, many different surgical approaches exist to arrive at this outcome. For the brow and upper-eyelid area, the surgical approaches include the following: (a) raising the brow through a browlift with or without upper blepharoplasty to remove redundant eyelid skin,
(b) performing an isolated upper-eyelid blepharoplasty, (c) fat enhancement of the brow, and (d) combining fat transfer with upper blepharoplasty. Selection of which procedure(s) is predicated on the patient’s anatomy and on what outcome the patient desires. With advancing age, there are several changes seen in the brow/upper-eyelid complex. The brow deflates due to loss of soft-tissue fullness. The loss of volume will result in skeletonization of the superior orbital rim and/or significant descent of the brow. The upper eyelid may demonstrate hooding of the eyelid skin and/or pseudoherniation of eyelid fat.
(b) performing an isolated upper-eyelid blepharoplasty, (c) fat enhancement of the brow, and (d) combining fat transfer with upper blepharoplasty. Selection of which procedure(s) is predicated on the patient’s anatomy and on what outcome the patient desires. With advancing age, there are several changes seen in the brow/upper-eyelid complex. The brow deflates due to loss of soft-tissue fullness. The loss of volume will result in skeletonization of the superior orbital rim and/or significant descent of the brow. The upper eyelid may demonstrate hooding of the eyelid skin and/or pseudoherniation of eyelid fat.
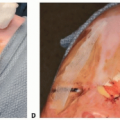
 Figure 2-1A, B, C: Preoperative view of a patient in her early 50s showing facial volume loss associated with aging. Her periorbital hollowing is much more evident on the profile and three-quarter oblique views. D: Postoperative view following fat transfer to the periorbital and midface regions shows aesthetic improvement in those areas. |
 Figure 2-2: Patient showing panfacial age-related volume loss. |
In our opinion, brow rejuvenation has too frequently relied on lifting procedures and has overlooked the importance of restoring volume. Upper-eyelid rejuvenation has traditionally been approached with aggressive removal of upper-eyelid orbital fat and skin. It is our contention that the overly elevated brow and aggressively sculpted upper-eyelid sulcus do not impart a youthful appearance but instead create either an aged appearance or a surgical look. In women, the increase in the length of the middle third of the face as a result of browlifting accentuates the unattractive rectangular facial appearance associated with aging, and skeletonization of the orbital rim removes the fullness necessary to attractively frame the eye. In men, exposing the orbital rim and upper-eyelid sulcus can give a feminized appearance (Fig. 2-3). We believe that the overuse of browlifting is in part due to surgeons allowing the available techniques to dictate the goals, rather than the aesthetic goals dictating the choice of procedure. Additionally, patients often misunderstand the aging process and request these types of changes. Reviewing a patient’s photographs when he or she was young can be instructive for both the patient and surgeon in planning a strategy for creating a more youthful appearance. It is quite common when looking at these photographs to realize that brow descent is dramatically less than the patient believes and that loss of volume in the brow with resulting skin hooding are the most significant changes.
The surgeon should strive not only to meet a patient’s aesthetic expectations but also ensure that the result will look natural, not surgical. A mildly ptotic brow that exhibits volume loss can be best addressed with a fat transfer and, if accompanied by dermatochalasis, an upper-eyelid blepharoplasty. Patients with a truly ptotic brow resting below the orbital rim will benefit from a browlift. The browlift violates tissue planes that preclude a concurrent fat transfer to the lateral superior orbital rim.
A sculpted brow/upper-eyelid complex can be seen as an attractive appearance but only if it is associated with a full inferior orbital rim and midface. Some of our patients
desire this appearance even if it is a change from the way they looked when they were younger. In these patients, it is critical to ensure that the inferior orbital rim and midface have adequate fullness either naturally or with fat transfer as part of the surgical plan.
desire this appearance even if it is a change from the way they looked when they were younger. In these patients, it is critical to ensure that the inferior orbital rim and midface have adequate fullness either naturally or with fat transfer as part of the surgical plan.
 Figure 2-3A: Preoperative view of a male patient who disliked the heaviness of his brow and wanted the effect of a browlift. B: The same patient is shown following browlift and a fat transfer to the cheeks. Note that the browlift has a tendency to feminize the patient’s face. |
 Figure 2-4A: This patient demonstrates a very hollow upper-eyelid sulcus with skeletonization of her superior orbital rim. B: Postoperative view following facelift and fat transfer that included placement along her superior orbital rim and upper eyelid in order to de-emphasize the hollow upper-eyelid sulcus. Although she was ultimately quite happy with the result, this photograph shows residual postoperative edema in the right upper-eyelid/brow region, which bothered her even after all other edema had effectively resolved. |
Upper Eyelid
The patient with upper-eyelid hollowing and a deep eyelid sulcus secondary to aging or prior surgery should be carefully approached. Unless the patient explicitly desires correction of this problem, the surgeon should avoid suggesting aggressive fat transfer to the upper-eyelid orbital region as part of the periorbital fat grafting plan (Fig. 2-4). Again, it is important to establish what the patient is displeased with, and in some cases, the hollowed upper eyelid is not an attribute the patient wants corrected. As opposed to fat transfer to the lateral brow (described in Chapter 3 as part of the volumetric foundation), which is technically straightforward and requires little recovery time, fat transfer to the inferior aspect of the superior orbital rim and/or the central upper-eyelid hollow can be technically challenging (described as an advanced technique in Chapter 3) and is associated with a prolonged recovery period of weeks to months during which time the patient often feels that the upper eyelid has an unnatural appearance. Only with patient prompting and explicit preoperative consultation should a surgeon decide to proceed with aggressive fat transfer to address a hollowed upper eyelid.
Temple
A hollowed temple may impart an unhealthy and/or aged appearance and should be evaluated for fat transfer. Temporal fat transfer can be technically challenging (described as an advanced technique in Chapter 3) and should generally only be undertaken once the surgeon has greater experience with fat transfer. Browlift procedures and facelift procedures with extension into the temporal region preclude simultaneous temporal fat transfer.
Midface
The midface is often the most important area for fat transfer because it provides the essential frame for the eye. Of all the facial highlights that accentuate the youthful
appearance, it is the highlight of the full lateral cheek that is associated with a beautiful and youthful face. A full cheek is a critical element in creating the ideal heart-shaped face, as described in Chapter 1. The cheek should transition smoothly into the lower eyelid. A youthful countenance does not exhibit separation between these two areas, and the goal for fat transfer should be to reunite the lower eyelid and cheek (Fig. 2-5).
appearance, it is the highlight of the full lateral cheek that is associated with a beautiful and youthful face. A full cheek is a critical element in creating the ideal heart-shaped face, as described in Chapter 1. The cheek should transition smoothly into the lower eyelid. A youthful countenance does not exhibit separation between these two areas, and the goal for fat transfer should be to reunite the lower eyelid and cheek (Fig. 2-5).
 Figure 2-5A, B: This patient had a transconjunctival blepharoplasty with fat transfer to the lower eyelid and cheek, achieving the ideal youthful convexity of the lower eyelid/cheek complex. |
Inferior Orbital Rim
The degree of lower-eyelid fat protrusion should be carefully inspected. Typically, most individuals experience only limited middle and medial fat protrusion. Although any kind of blepharoplasty is appropriate for management of lower-eyelid fat protrusion, a transconjunctival blepharoplasty has proven to be ideal in our hands due to the preservation of tissue planes, which permits concurrent fat transfer and is associated with a minimal incidence of lower-eyelid malposition. Some fat transfer surgeons advocate fat augmentation alone to fill the inferior orbital rim hollow, feeling there is no need for a blepharoplasty. In patients without significant fat protrusion, this is a reasonable approach (Fig. 2-6). In the presence of more than minimal pseudoherniated lower-eyelid fat, the volumes required to establish a confluence between the lower eyelid and cheek without concurrent lower-eyelid blepharoplasty can be considerable and predispose toward contour irregularities. If fat transfer alone is performed in such a patient and a smooth contour is achieved, there is risk that the patient may feel there is too much fullness of his or her lower eyelid, necessitating a second procedure to perform a blepharoplasty to reduce this fullness. Therefore, appropriate fat reduction of the lower eyelid combined with fat transfer to the inferior orbital rim can achieve a predictable attractive appearance to this area (Fig. 2-7). With the goal of maximizing the surgical result and minimizing the need for touch-up procedures, in the presence of visible lower-eyelid fat pseudoherniation, a lower-eyelid transconjunctival blepharoplasty should be combined with fat transfer. The exception to this rule may be the patient with a prominent, negative-vector eye and malar hypoplasia, where periorbital fat removal will accentuate the prominence of the eye and further subtract away an adequate frame for the eye.
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


