34 Preoperative Donor Evaluations
Summary
Keywords: laxity elasticity safe donor area hair mass index cross-section trichometer folliscope hair density follicular density donor density densitometer
Key Points
•Evaluate donor qualities through physical examination, patient history, both personal and family, and stay within safe donor area (SDA).
•Measure the vellus-to-terminal hair ratio to evaluate for possible diffuse unpatterned alopecia (DUPA).
•Avoid excessive wound tension by preoperatively measuring the laxity of the scalp.
34.1 Introduction
All hair transplant procedures begin with removing hair from the donor region and transplanting it to recipient areas of need. Limmer first popularized taking a tapered ellipse from the donor region.1 Since the donor area is limited in all patients—to a lesser or greater extent—it is a limited commodity. Therefore, the donor must be treated with the utmost respect and care. Hair restoration surgeons (HRS) need to strive to maintain its integrity and use as little as possible to produce the desired result.
Patient selection is critical and in this chapter the focus is to determine what result we can predict based on available donor hair using an elliptical harvest method and the area to be covered. FUE may also be used in conjunction with strip harvest to somewhat expand the available donor hair, but this is covered in other chapters. It is critical to first identify the patient’s expectations and then present an honest prediction of the kind of results that can be achieved. This discussion should be documented as accurately as possible in writing, with pictures or computer modeling, or other methods. Objective and subjective data are gathered and then evaluated to provide the optimal result for each patient who comes for advice. See Video 34.1 and Video 34.2 on the fundamentals of strip harvesting, assessment, and planning.
34.2 Initial Patient Medical History
The simple but extremely difficult task that each HRS must perform on initial evaluation is the prediction of future hair loss, especially relating to the safe donor area (SDA).2,3 What is the patient going to look like with no medical or surgical therapy when he or she is 60 to 70 years old? The key factors in the history include age of onset of hair loss, rate or progression, and family history, particularly father, brothers, and both grandfathers. Also important are any medical illnesses or traumas that may have influenced hair loss, in particular anemia, thyroid disorders, malignancies, chemotherapy, medications associated with alopecia, scalp disorders, and any tendency toward keloid formation.
One must know the use of any medical therapies that proved helpful or not, that is, minoxidil (oral or topical), finasteride (oral or topical), photobiomodulation, platelet-rich plasma (PRP), and other hair loss treatments. These can be taken into consideration, but the permanent surgical plan should be determined based on worst-case scenario for the long-term pattern of alopecia.
34.3 Physical Examination
The physical characteristics of the donor area to be assessed include hair shaft caliber and texture, hair–skin color contrast, density of hair and follicular units (FUs), and percent of miniaturized hair compared to terminal hair.
If the hair is long enough, a hair mass index (HMI) measurement can be obtained.4,5,6 The scalp must also be evaluated for thickness, laxity, quality of previous surgery, and of course degree of hair loss. Of particular interest is any tendency toward keloid formation, which is more common in individuals with increased skin pigmentation. If there is any suspicion for keloid formation, it is advisable to do a small test procedure and observe for 6 to 9 months.
The HRS must evaluate the entire scalp including the donor area for diseases such as psoriasis and alopecia areata, as well as scarring alopecias including lichen planopilaris, discoid lupus, frontal fibrosing alopecia, and chronic folliculitis. For details of these and other scalp pathology, refer to Chapters 8 and 9.
To summarize, the physical examination must support the diagnosis of androgenetic alopecia, qualify the patient for hair restoration surgery, and should allow the HRS to estimate the safe length and width of strip to remove for the desired coverage.
34.4 Safe Donor Area
One of the founding principles of hair restoration surgery is to select donor hair that will grow “permanently” in the recipient area. However, one must not claim that this hair will “last the rest of your life” or that it is “permanent,” but rather convey the concept that donor hair will follow the same history with aging as if it had been left in the donor area.
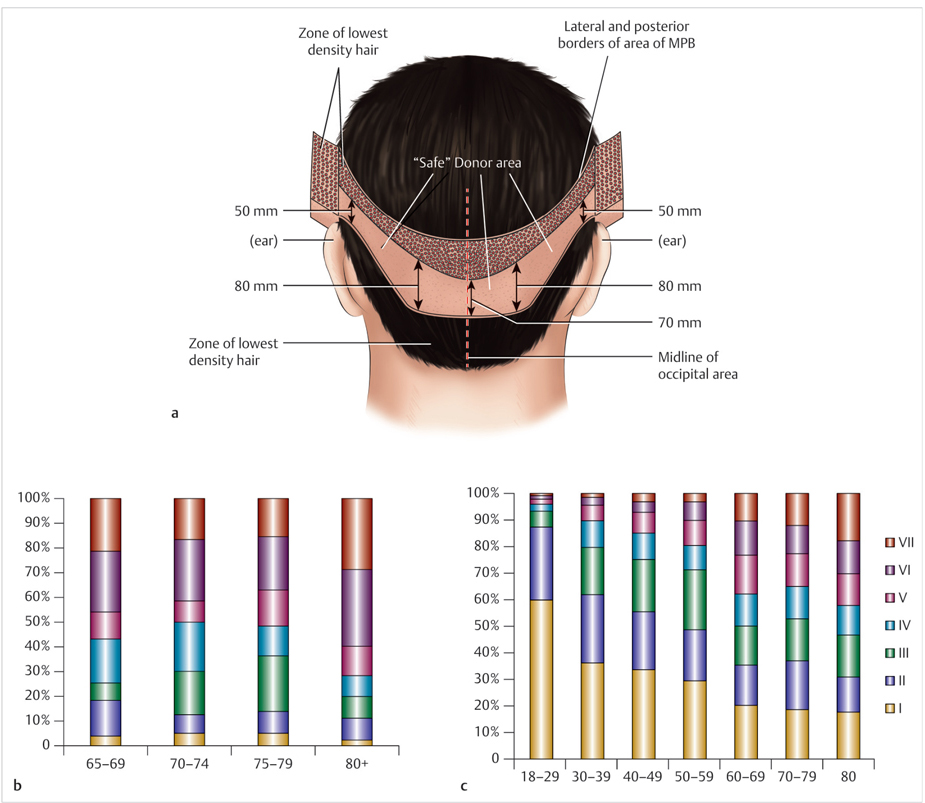
One should follow the guidelines determined by the historic observations made by Alt and studies by Unger in defining the boundaries of the SDA.2,3 Alt defined the SDA as the hair found in the safe fringe that persists on the sides and posterior scalp in patients who attain extensive male-pattern alopecia, usually 6.5 to 7.0 cm wide and narrowing toward the occiput (Fig. 34.1). This area is bounded anteriorly by a vertical line drawn from the external auditory canal. Density anterior to this line is generally insufficient to allow extensive harvesting. In addition, the posterior branch of the superficial temporal artery traverses this region. Since this artery supplies the major portion of the afferent blood supply to the superior and anterior portion of the scalp, compromising this vessel may have a detrimental effect on graft growth in this area. A horizontal line is drawn from a point 2 cm above the reflection of the skin of the external ear and scalp. The horizontal line is then carried from this point posteriorly to the midline of the occiput, which defines the superior border of the SDA. Alt counseled that 2.5 cm of the fringe hair should remain above the scalp for camouflage.2 Unger extended the vertical line from the anterior auditory canal anteriorly 28 mm (Fig. 34.2a). His SDA was based on a study of 328 men older than 65 years. They were subdivided into several groups: 65- to 69–year-olds, 70- to 74-year-olds, and older than 80 years; 80% of these men younger than 80 years fit into his definition of SDA, which is reassuring (Fig. 34.2b, c).
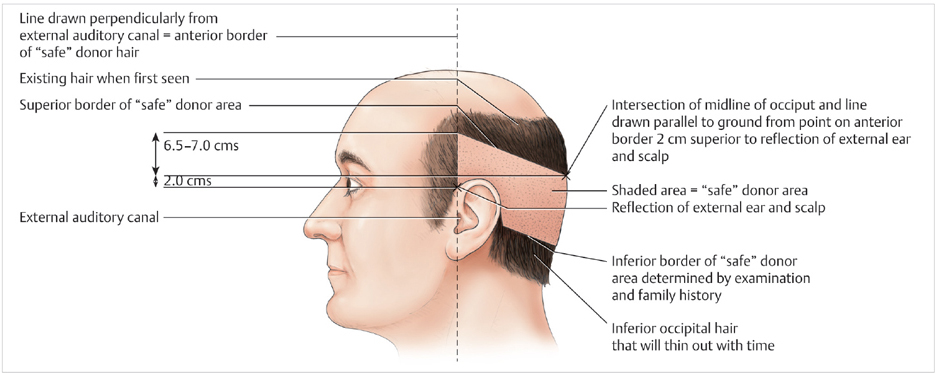
Fig. 34.1 Alt’s safe donor area.
The inferior and superior boundaries are difficult to define since the HRS cannot precisely predict ultimate hair loss. On the average, the SDA will measure 6.5 to 7.0 cm from the edge of the anticipated fringe.2,3 A more detailed measurement of 216 men with type III to VI Norwood male-pattern baldness is described for the anterior, temporal, parietal, and occipital area (Table 34.1).7 This SDA extends in a curvilinear fashion dropping from the supra-auricular area posterior and inferior to the center of the occiput. The incision should always be placed greater than 2 cm from the edge of the anticipated fringe so there is adequate hair to shingle over the scar.
Table 34.1 Average height (mm) of acceptable donor area from 216 patients with type III, IV, V, and VI Norwood male-pattern baldness (by Unger)
65–69 y | 70–74 y | 75–79 y | >80 y | |
Anterior | 33 | 24 | 29 | 22 |
Temporal | 80 | 55 | 62 | 59 |
Parietal | 97 | 76 | 79 | 81 |
Occipital | 86 | 60 | 69 | 62 |
If subsequent surgeries are performed, it is standard practice to remove the previous scar8 and take new donor tissue from the same most permanent region of the fringe. It is important to excise a narrower section over the mastoid, where elasticity is lower. Subsequent surgeries will usually produce 25 to 30% fewer FUs than the first surgery if near maximum excision was performed in the first surgery. This decreased yield is due to three factors: decreased density, excision of alopecic scar tissue, and less scalp elasticity. If multiple scars are introduced (not an advisable strategy), circulation and hair growth can be compromised (Fig. 34.3). The donor may also be compromised if one neglects to evaluate for keloid formation (Fig. 34.4).
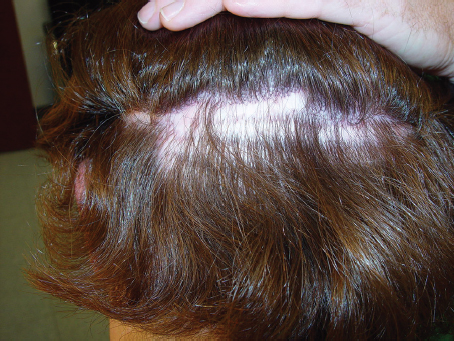

Fig. 34.4 Donor keloid scar.
34.5 Recipient Area Requirements
This important issue is covered in an earlier Chapter 20, but there are some rather simple guidelines to consider because once the goals of the patient have been identified one must determine approximately how many FUs will be required to give a reasonable appearance of density.9,10 Several authors suggest that 30 to 40 FUs/cm2 gives a reasonable appearance of density.
There are various templates to help calculate FU requirements.11,12,13 The Jimenez, Chang, Farjo–Cole, and the Devroye methods are all excellent, but in the author’s experience the most helpful method is using his premeasured palmer surface of the hand. The author’s hand works well as a measuring tool. The volar surface of his fingers is 40 cm2 and the palm is 100 cm2. Since the hand is rarely misplaced, it is placed on the scalp and very quickly the HRS can estimate the area in square centimeter, which needs coverage. Therefore, by multiplying this estimated area by the 20 to 40 FUs/ cm2, one can determine quickly the number of FUs needed for reasonable coverage.
34.6 Hair Density Terminology
Definition of terms is critical for recording of donor density data and communication between HRS. This information is critical in estimating the amount of hair and area of strip to perform the desired hair transplant surgery.
The first is hair density (HD), which is the number of hairs in a defined surface area. This is usually defined as the number of hairs per square centimeter. The second is follicular unit density (FUD). This is the number of FUs in a given surface area, usually 1 cm2. The third is calculated density (CD), which is the number of hairs per FU. This is an average based on multiple donor evaluation sites (Fig. 34.6).
•Hair density (HD) = total number of hairs in a defined surface (hair/cm2).
•Follicular density (FUD) = total number of FUs in a defined surface area (FUs/cm2).
•Calculated density (CD) = D/FUD = hairs/FU.
•Total number of hairs transferred (THT) = (mean HD) (cm2 excised).
Related posts:
 Hair Anatomy and Histology for the Hair Transplant Surgeon
Hair Anatomy and Histology for the Hair Transplant Surgeon
 Plugged in: How to Ensure That Your Practice Thrives (and Survives) in Today’s DigitalWorld
Plugged in: How to Ensure That Your Practice Thrives (and Survives) in Today’s DigitalWorld
 Transplanting into Areas of Cicatricial Alopecia
Transplanting into Areas of Cicatricial Alopecia
 Special Considerations for Postoperative Care in Follicular Unit Excision
Special Considerations for Postoperative Care in Follicular Unit Excision
 Hairline and Recipient Area Repair of Poor Previous Transplantation
Hairline and Recipient Area Repair of Poor Previous Transplantation
 Ergonomics in Hair Restoration Surgery: FUE Technique
Ergonomics in Hair Restoration Surgery: FUE Technique
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


