The double “S” principle should be followed for facial reconstruction: the “ similarity” of the donor site to the defect area and the reconstruction should be based on the different “ subunits” of the face. In this article the pre-expanded, bipedicled supratrochlear perforator flap method is described, which is used for the resurfacing of both nasal and upper lip defects. This method can provide 2 independent flaps with sufficient tissue from 1 single donor site, resurfacing the nasal and upper lip units separately and providing an unparalleled color and texture match and ideal reconstructive result.
Key points
- •
The supratrochlear perforator vessels come in pairs in the forehead, which permit 2 flaps to be harvested at the same time.
- •
The forehead is an excellent source of skin and soft tissue for most nasal reconstruction. Because the upper lip is adjacent to the nose, the forehead should be a possible donor site for upper lip reconstruction.
- •
The pre-expanded, bipedicled supratrochlear perforator flap technique allows the reconstruction of the nose and the upper lip, 2 independent units, with 2 flaps from 1 donor site.
- •
The pre-expansion technique can provide abundant tissue so that the donor site can be closed directly after the 2 flaps are harvested. Meanwhile, the pre-expansion is a flap delay procedure that can enhance the blood perfusion of the flaps, especially in their distal parts.
Introduction
The nose and upper lip are 2 adjacent units in the middle of the face that have prominent aesthetic status for humans. Defects in these 2 units are extremely conspicuous. The nose and upper lip are 2 projecting structures in the face, hence are prone to be damaged in trauma, or flame or chemical burns and also can be violated by tumor and infections. On the other hand, they tend to be destroyed together because of their adjacent positions. Simultaneous reconstruction of the 2 central facial units is a complex and challenging issue for plastic surgeons.
The principles of replacing “like with like” and achieving a unit or subunit reconstruction is well established. In 1956, Gonzalez-Ulloa described the regional aesthetic “units” of the face, based on skin thickness, to emphasize the need for restoring facial skin units in complete regions as opposed to patch work. Burget and Menick developed the facial “units” principle and also divided the nose into “subunits” based on skin quality, border outline, and 3-dimensional contour. They looked at facial surfaces as convex and concave regions that allow for different light reflection. Burget and Menick emphasized that if a graft or a suture line is matched to the shape of a subunit, the natural appearance of facial light and shadows can be restored. Indeed, following the “units” and “subunits” concept, an optimal reconstructive result can be achieved because the scars are hidden within the joints between units or subunits and perceived as normal facial topography. More importantly, myofibroblasts lie in the recipient site under the transferred flap. They will contract, causing the transposed skin flap to rise above the level of adjacent skin. The flap will appear as a distracting patch if the defect is filled without regard to the subunit outline. When an entire subunit is resurfaced, the pincushioned flap shrinkwraps could augment, rather than distort, the contour of a subunit. The authors summarize these concepts and put forward the concept of the double “S” principle (similarity and subunit) for the facial reconstruction. The first “S” stands for the “ similarity” of the donor site to the defect area and the second “S” means the reconstruction should be based on the different “ subunits” of the face. Performing facial reconstruction according to this principle can dramatically improve the final appearance of facial scars and surgical outcomes.
Many techniques have been described in the literature for the reconstruction of nose and upper lip defects. The easiest approach to resurfacing facial soft tissue defects is skin grafting. However, this method should generally be avoided because of the hyperpigmentation, secondary contracture, and poor texture. Free flaps can act as workhorse flaps in reconstruction for acute wounds and defects after trauma or tumor resection, but their poor color and texture matching are the main reasons and patients very often need a second or third or even more revisions to improve cosmetic outcome. Most of the reports are focused on the forehead flap for the reconstruction of nose and local flaps for the reconstruction of the upper lip. However, multiple donor sites are required and local flaps can resurface only small defects. Moreover, patients with composite nasal tissue losses often have facial injuries around the defect, reducing the availability of the donor site. Thus, it may be difficult to find an appropriate local flap for upper lip reconstruction. Yoshihiro and colleagues reported their technique of using the split-scalping forehead flap for the reconstruction of defects of the nose and upper lip. This technique reduced the number of donor sites but the cosmetic of hemi-forehead donor site was unpleasant and required skin grafting. Because the forehead area is an excellent source of skin and soft tissue for most nasal reconstructions in clinical practice, and it also has the superior color and texture match to the facial skin, the forehead area should be a possible donor site for both nose and upper lip reconstruction. Based on the work of pioneers and the anatomic features of the facial vessels, which come in pairs, we present our experience with the pre-expanded, bipedicled supratrochlear perforator flaps for simultaneous nasal and upper lip resurfacing. This novel approach allows the reconstruction of multiple facial subunits with tissue of similar color and texture to the recipient site from a single donor site.
Introduction
The nose and upper lip are 2 adjacent units in the middle of the face that have prominent aesthetic status for humans. Defects in these 2 units are extremely conspicuous. The nose and upper lip are 2 projecting structures in the face, hence are prone to be damaged in trauma, or flame or chemical burns and also can be violated by tumor and infections. On the other hand, they tend to be destroyed together because of their adjacent positions. Simultaneous reconstruction of the 2 central facial units is a complex and challenging issue for plastic surgeons.
The principles of replacing “like with like” and achieving a unit or subunit reconstruction is well established. In 1956, Gonzalez-Ulloa described the regional aesthetic “units” of the face, based on skin thickness, to emphasize the need for restoring facial skin units in complete regions as opposed to patch work. Burget and Menick developed the facial “units” principle and also divided the nose into “subunits” based on skin quality, border outline, and 3-dimensional contour. They looked at facial surfaces as convex and concave regions that allow for different light reflection. Burget and Menick emphasized that if a graft or a suture line is matched to the shape of a subunit, the natural appearance of facial light and shadows can be restored. Indeed, following the “units” and “subunits” concept, an optimal reconstructive result can be achieved because the scars are hidden within the joints between units or subunits and perceived as normal facial topography. More importantly, myofibroblasts lie in the recipient site under the transferred flap. They will contract, causing the transposed skin flap to rise above the level of adjacent skin. The flap will appear as a distracting patch if the defect is filled without regard to the subunit outline. When an entire subunit is resurfaced, the pincushioned flap shrinkwraps could augment, rather than distort, the contour of a subunit. The authors summarize these concepts and put forward the concept of the double “S” principle (similarity and subunit) for the facial reconstruction. The first “S” stands for the “ similarity” of the donor site to the defect area and the second “S” means the reconstruction should be based on the different “ subunits” of the face. Performing facial reconstruction according to this principle can dramatically improve the final appearance of facial scars and surgical outcomes.
Many techniques have been described in the literature for the reconstruction of nose and upper lip defects. The easiest approach to resurfacing facial soft tissue defects is skin grafting. However, this method should generally be avoided because of the hyperpigmentation, secondary contracture, and poor texture. Free flaps can act as workhorse flaps in reconstruction for acute wounds and defects after trauma or tumor resection, but their poor color and texture matching are the main reasons and patients very often need a second or third or even more revisions to improve cosmetic outcome. Most of the reports are focused on the forehead flap for the reconstruction of nose and local flaps for the reconstruction of the upper lip. However, multiple donor sites are required and local flaps can resurface only small defects. Moreover, patients with composite nasal tissue losses often have facial injuries around the defect, reducing the availability of the donor site. Thus, it may be difficult to find an appropriate local flap for upper lip reconstruction. Yoshihiro and colleagues reported their technique of using the split-scalping forehead flap for the reconstruction of defects of the nose and upper lip. This technique reduced the number of donor sites but the cosmetic of hemi-forehead donor site was unpleasant and required skin grafting. Because the forehead area is an excellent source of skin and soft tissue for most nasal reconstructions in clinical practice, and it also has the superior color and texture match to the facial skin, the forehead area should be a possible donor site for both nose and upper lip reconstruction. Based on the work of pioneers and the anatomic features of the facial vessels, which come in pairs, we present our experience with the pre-expanded, bipedicled supratrochlear perforator flaps for simultaneous nasal and upper lip resurfacing. This novel approach allows the reconstruction of multiple facial subunits with tissue of similar color and texture to the recipient site from a single donor site.
Treatment goals and planned outcomes
To improve the final appearance of facial scars and surgical outcomes, we put forward a concept of double “S” principle (similarity and subunit) for the facial reconstruction. The first “S” stands for the “ similarity” of the donor site to the defect area and it is a selection criteria of the best donor site in reconstructive surgery. The forehead region should be the optimal choice owing to the neighborhood relationship and similar color and texture to the nose and upper lip. The second “S” means the reconstruction should be based on the different “ subunits” of the face so as to restore facial skin unit or subunit with the same tissue and hide the scars within the joints between units or subunits. The nose and upper lip should be restored separately because they belong to different units of the face.
Based on the double “S” principle and with the help of tissue expansion technique, we applied the pre-expanded bipedicled supratrochlear perforator flap for simultaneous reconstruction of the nasal and upper lip defects from a single donor site. With the experience of more than 30 cases, we think that this technique is simple and safe in achieving excellent aesthetic results in nasal and upper lip reconstruction. When properly planned and performed, this operation can also obtain a low complication rate and minimal donor site morbidity.
Preoperative planning and preparation
Patients with burn scar contractures of the nose and upper lip were operated on with the pre-expanded, bipedicled supratrochlear flap in our department ( Fig. 1 ). All operations were performed by the senior author (YXZ) under general anesthesia. A detailed informed consent about the operative technique, surgical risks, and potential complications were signed by the patients. The preoperatively photograph included full-face and both frontal and lateral views. Facial radiographs, computed tomography scans, or MRI are occasionally needed to clarify bony and soft tissue defects to the midface. The patients were asked to take a bath before the operation and a usual prophylactic antibiotic administration was done preoperatively.
Procedural approach
The operation is performed under general anesthesia, avoiding the distortion created by local anesthesia or the chemical blanching of epinephrine.
Stage 1: Expander Placement
A silicone tissue expander is inserted into the subgaleal plane of the forehead. The access incision is placed 1 to 2 cm within the hairline with the pocket extended from the hairline to the supraorbital rims bilaterally. Both the subgaleal pocket and the tissue expander are irrigated with antibiotic solution. The rectangular expander size ranges from 100 to 200 mL with the remote injection port embedded in the scalp. Twenty percent of the expander volume is inflated through the injection at the time of the expander placement so as to maintain some tension on the newly created pocket. A closed suction drainage is used for 1 to 2 days.
The expansion process begins 2 weeks postoperatively. Using saline solution and a 23-gauge hypodermic needle, 10% to 20% of the expander volume is injected twice a week until a final volume of 2.5 times the expander capacity is reached. A full expansion can be achieved usually in 3 months.
Stage 2: Flap Transfer
All the important landmarks and reference points are identified and marked before the first incision. The hairline, eyebrows, the outline of the nasal and upper lip units or subunits, and the margin of the scar are all marked with ink. The entire scar tissue around the nose and upper lip is removed. The release of the scars is considered complete only when all the landmarks return in their normal anatomic position. Until then, the exact sizes of defects of nose and upper lip could be measured. The reconstruction should follow the principle of unit/subunit, so not only the scar itself but also healthy tissue in the same unit/subunit is removed. Two templates are designed based on the size of the nose and upper lip defects.
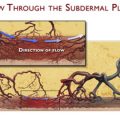
Two independent supratrochlear artery perforator flaps are then marked side by side on the expanded forehead tissue. The 2 flaps have an axial pattern blood flow of which the supratrochlear vessels are the primary supply, and the anastomoses of the dorsal nasal, supraorbital, and angular arteries are the secondary supply ( Fig. 2 ). This secondary nourishment increases the flap’s consistent blood supply and the proximal two-thirds of the pedicle may be quite narrow while the remaining part of the flap is extended to incorporate all the previously expanded skin area. The robust blood supply of the forehead area frees us from the concerns about the survival of the distal portion of the flap, so more attention can be paid to the reconstruction of defects. The bases of the 2 flaps are at the orbital margin, near the medial end of the eyebrow. The 2 pedicles should lie side by side in the glabella area and be marked 1.2 to 1.5 cm in width to allow an arc of rotation of 180° to cover the nasal or upper lip defect without any torsion or kinking of the vessels. One flap is designed in a trilobed fashion and is used for nasal defect resurfacing. Another flap, based on the contralateral supratrochlear vessels, is marked longer than the first one and with an “L” shape to ease the placement of the pedicle beside the nose when it rotates to cover the defect of the upper lip. In addition, a curved distal edge is incorporated in the flap component to reflect the convexity of the upper lip. The dimensions of the flaps are planned accurately by the use of the templates. The flap sizes are approximately increased by 0.5 cm on each side to prevent the distortion of tissues at the time of contracture during the healing process. The length of the flap depends on the distance from the pivot point of the orbital margin to the recipient site. If a longer pedicle is needed, the pivot point of the flap could be lowered toward the medial canthus and closer to the defect. Another way to achieve a longer pedicle is to place the flap more distally within the hairline, although a small amount of hair at the distal end of the flap is included. In female patients, hair could be removed later with laser or other procedures, whereas in male patients the hair on the flap can simulate the moustache. Attention should be paid that excessive tension (the flap is too short or too small, the pedicle is too wide or twisted) can devascularize the flap and cause ischemia.