Early detection remains the most important strategy to reduce melanoma mortality. The identification and evaluation of new or changing skin lesions are important components of melanoma screening and are best performed today using complementary noninvasive imaging technologies, such as total body photography (TBP), dermoscopy, sequential digital dermoscopic imaging (SDDI), and reflectance confocal microscopy (RCM). Despite strong evidence showing that these screening techniques improve diagnostic accuracy for melanoma, they are not widely used by dermatologists. In this practice gaps review, the authors highlight the use, evidence, and rationale for TBP, dermoscopy, SDDI, and RCM.
Key points
- •
Good practices for melanoma diagnosis include strategies to detect new or changing skin lesions.
- •
Dermoscopy, total body photography, sequential digital dermoscopy imaging, and reflectance confocal microscopy are at present most relevant to identifying and evaluating new or changing skin lesions.
- •
The use of these noninvasive imaging technologies is particularly useful when screening individuals with high melanocytic nevus counts and atypical/complex nevus phenotypes for melanoma.
- •
Barriers such as lack of training and confidence, personal beliefs, and economical and logistical constraints have prevented the widespread use of those tools.
- •
Patient-driven health care aided by technology and complemented by teledermatology will likely rapidly alter the landscape of melanoma screening within the next decade.
Importance of new or changing melanocytic lesions
Despite increased public awareness of skin cancer and of the harmful effects of ultraviolet radiation (UVR), cutaneous melanoma incidence and mortality continue to increase in the United States. In 2015, approximately 73,870 people will be diagnosed with and 9940 will die of invasive melanoma. Although there have been recent improvements in the treatment of metastatic melanoma, early detection remains the most important strategy to reduce mortality. Evidence supporting this approach includes the recent population-based screening efforts in Germany, with initial results in the state of Schleswig-Holstein suggesting a nearly 50% decrease in melanoma mortality associated with skin cancer screening through total body skin examinations (TBSEs).
Many factors are recognized as important to the diagnosis of melanoma, including the identification of new or changing lesions. In 2004, the letter “E” was appended to the ABCD (Asymmetry, irregular Borders, more than one or uneven distribution of Color, or a large [greater than 6 mm] Diameter) mnemonic to highlight the importance of change in a melanocytic lesion as an important diagnostic criterion of melanoma. Similarly, the Glasgow 7-point checklist places significant importance on changes in size, shape, and color of skin lesions as major signs of melanoma. The fact that most melanomas (∼65%) arise de novo and are not contiguously associated with a melanocytic nevus underscores the importance of identifying new lesions in addition to changing lesions during TBSEs to maximize diagnostic sensitivity for melanoma. As the associated potential harms of skin cancer screening, in particular overdiagnosis, are increasingly recognized, identification of truly dynamic lesions with real potential for progression to metastatic and fatal disease may have the greatest short-term potential to limit harvesting of indolent and/or nonprogressive cancers.
Emphasis on detection and subsequent biopsy of changing skin lesions, however, may lead to a decrease in diagnostic accuracy for melanoma. A surrogate marker of positive predictive value is number needed to excise (NNE), which is the number of benign melanocytic lesions removed for every confirmed melanoma. Estimates in Europe and the United States of the NNE in children and adolescents are reported to range from 594 to 696, which are attributed to relying on change alone as an indication for biopsy. Nevogenesis is recognized as a highly dynamic process during life, with significant nevus volatility in younger individuals (ie, nevus growth, appearance, and disappearance). Even in adults, change alone in a skin lesion is not specific for the diagnosis of melanoma, and the appearance of new nevi is relatively common. Conditions such as body growth, weight gain, pregnancy, or UVR exposure can also lead to recognized benign changes in melanocytic lesions.
Importance of new or changing melanocytic lesions
Despite increased public awareness of skin cancer and of the harmful effects of ultraviolet radiation (UVR), cutaneous melanoma incidence and mortality continue to increase in the United States. In 2015, approximately 73,870 people will be diagnosed with and 9940 will die of invasive melanoma. Although there have been recent improvements in the treatment of metastatic melanoma, early detection remains the most important strategy to reduce mortality. Evidence supporting this approach includes the recent population-based screening efforts in Germany, with initial results in the state of Schleswig-Holstein suggesting a nearly 50% decrease in melanoma mortality associated with skin cancer screening through total body skin examinations (TBSEs).
Many factors are recognized as important to the diagnosis of melanoma, including the identification of new or changing lesions. In 2004, the letter “E” was appended to the ABCD (Asymmetry, irregular Borders, more than one or uneven distribution of Color, or a large [greater than 6 mm] Diameter) mnemonic to highlight the importance of change in a melanocytic lesion as an important diagnostic criterion of melanoma. Similarly, the Glasgow 7-point checklist places significant importance on changes in size, shape, and color of skin lesions as major signs of melanoma. The fact that most melanomas (∼65%) arise de novo and are not contiguously associated with a melanocytic nevus underscores the importance of identifying new lesions in addition to changing lesions during TBSEs to maximize diagnostic sensitivity for melanoma. As the associated potential harms of skin cancer screening, in particular overdiagnosis, are increasingly recognized, identification of truly dynamic lesions with real potential for progression to metastatic and fatal disease may have the greatest short-term potential to limit harvesting of indolent and/or nonprogressive cancers.
Emphasis on detection and subsequent biopsy of changing skin lesions, however, may lead to a decrease in diagnostic accuracy for melanoma. A surrogate marker of positive predictive value is number needed to excise (NNE), which is the number of benign melanocytic lesions removed for every confirmed melanoma. Estimates in Europe and the United States of the NNE in children and adolescents are reported to range from 594 to 696, which are attributed to relying on change alone as an indication for biopsy. Nevogenesis is recognized as a highly dynamic process during life, with significant nevus volatility in younger individuals (ie, nevus growth, appearance, and disappearance). Even in adults, change alone in a skin lesion is not specific for the diagnosis of melanoma, and the appearance of new nevi is relatively common. Conditions such as body growth, weight gain, pregnancy, or UVR exposure can also lead to recognized benign changes in melanocytic lesions.
Current best practice
Good practices for melanoma diagnosis therefore include, but are not limited to, strategies to detect new and/or changing lesions and to determine if these findings warrant skin biopsy. The use of noninvasive imaging technologies, such as dermoscopy, total body photography (TBP), sequential digital dermoscopy imaging (SDDI), and reflectance confocal microscopy (RCM), are at present most relevant to identifying and evaluating new and changing skin lesions during screening examinations, particularly in individuals with high melanocytic nevus counts and atypical/complex nevus phenotypes.
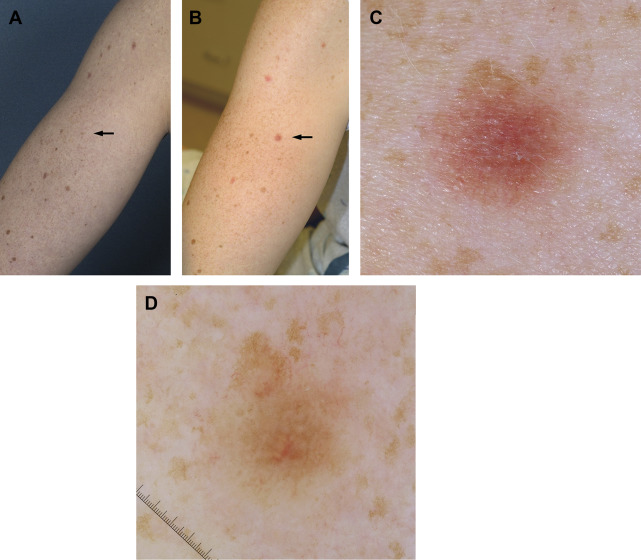
Use of TBP images by physicians and patients during TBSEs and skin self-examinations (SSEs), respectively, allow for identification of new lesions and macroscopic changes in existing skin lesions ( Fig. 1 ). Physicians who routinely use TBP during skin examinations argue that its use improves sensitivity and specificity for melanoma detection. Use of TBP images during SSEs has been shown to improve patients’ confidence in performing SSEs and to increase patients’ sensitivity for detection of new or changing skin lesions compared with performance of SSE alone without access to TBP images.
After recognition of a new or changing skin lesion with TBP, dermoscopic evaluation is the next most appropriate step in evaluation. Meta-analyses have demonstrated that the use of dermoscopy by trained evaluators improves diagnostic accuracy for melanoma detection. Access to dermoscopy reduces unnecessary biopsies of skin lesions because most pigmented lesions will conform to a recognized benign nevus pattern. The predominant nevus pattern depends on age, skin type, and the interaction between genes and the environment, such as UVR exposure. In the context of patients with many nevi, use of the dermoscopic comparative examination and the ugly duckling concept will prevent unnecessary biopsies of nevi. Lesions with features concerning for melanoma should undergo biopsy, whereas those with equivocal but not diagnostic features could undergo SDDI and/or interrogation with RCM.
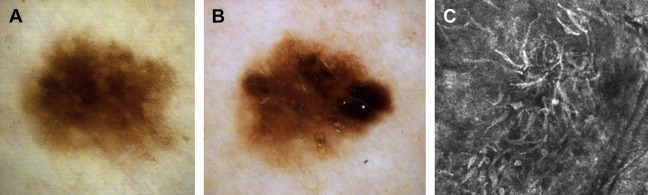
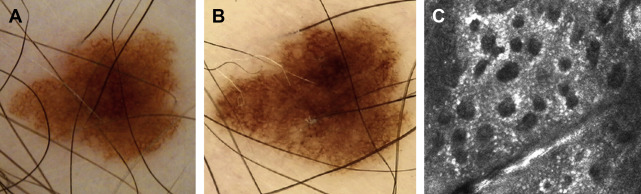
SDDI involves capturing dermoscopic images of lesions over time in order to identify changes concerning for melanoma and can be used in 2 complementary ways. The first method involves repeating dermoscopic images of skin lesions at regular intervals for detailed comparative analysis, which when combined with TBP has been referred to as “digital follow-up” and has been shown to enable recognition of melanomas that lack diagnostic clinical or dermoscopic features at baseline evaluation ( Fig. 2 ). SDDI can also be used as a second-level screening evaluation of specific lesions with borderline features. When used in this manner, SDDI dramatically reduces the number of biopsies of benign lesions compared with use of dermoscopy alone ( Fig. 3 ). Access to SDDI compared with dermoscopy alone has also been associated with a 35% reduction in the cost per melanoma excised in a 1-year retrospective observational study in Belgium.
A 5-year prospective observation study of 311 patients in Australia at “extreme high risk” for melanoma demonstrates the complementary effectiveness of TBP, dermoscopy, and SDDI in the diagnosis of melanoma. After a median follow-up of 3.5 years, 70 of 75 primary melanomas detected in this cohort were either in situ or 1-mm or thinner invasive melanomas. Furthermore, 39.3% and 37.7% of after-baseline melanomas were detected exclusively or aided by SDDI and TBP, respectively. The very low NNE of 4.4:1 reflects that surveillance with this protocol did not lead to excess biopsies and compares favorably to recently published estimates of NNE in skin cancer specialist (8.7:1) and nonspecialist (29.4:1) clinics. Salerni and colleagues reported similar overall effectiveness in melanoma screening using TBP, dermoscopy, and SDDI in a 10-year retrospective observational study of 618 patients in Spain at high risk for melanoma. In this study, 53.3% (n = 53) of melanomas were in situ, and the median Breslow depth of invasive melanomas (n = 45) was 0.5 mm. Although neither study was designed to investigate if intensive screening for melanoma with these imaging techniques is associated with reduced mortality or melanoma overdiagnosis, these studies as well as a recent meta-analysis on the topic strongly suggest that the use of TBP, dermoscopy, and SDDI to identify and evaluate new or changing skin lesions permits early melanoma diagnosis at curable stages with low NNE ratios.
New or changing skin lesions with equivocal features after dermoscopic or SDDI examination can undergo analysis with RCM, which noninvasively allows for cellular assessment of the epidermis and superficial dermis at a resolution approaching histologic detail (see Fig. 2 ; Fig. 4 ). The reported sensitivity and specificity of RCM for melanoma among experts are estimated to range from 91% to 96.5% and 68% to 94.1%, respectively. Used as a second-level screening test, RCM has been shown to improve diagnostic accuracy for melanoma and to prevent unnecessary biopsies of benign lesions. RCM may be particularly useful for evaluation of amelanotic, facial, or dermoscopically nonspecific lesions. Studies have specifically demonstrated the impact of RCM as a screening evaluation after SDDI. In this setting, it can prevent nearly 70% of unnecessary biopsies of benign nevi found to have changes that warrant removal.
Relevant Dermoscopic Changes During Follow-up
Detected changes in melanocytic lesions must be interpreted depending on a patient’s phenotype, risk markers, and predominant dermoscopic pattern. The interval of change is particularly relevant; any short-term (0–3 months) change in a lesion on an adult should be of concern and biopsy strongly considered. Exceptions could include physiologic changes during pregnancy or pubertal growth, recent intense UVR exposure, or laser depilation.
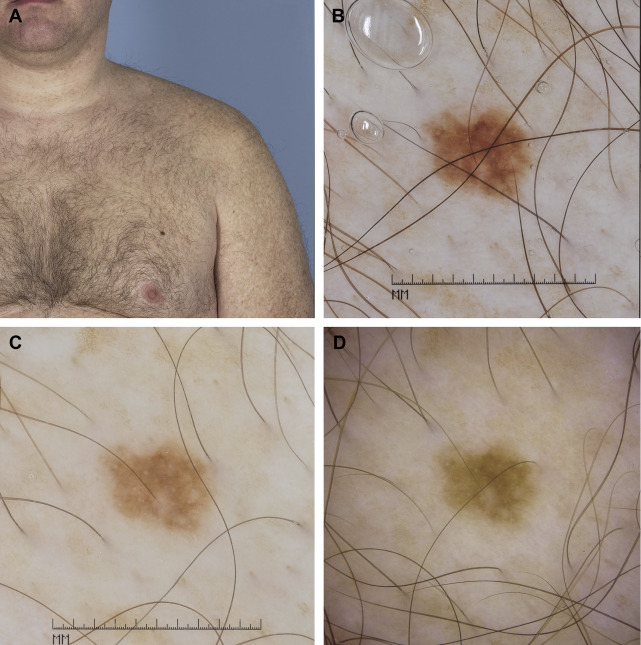
Nevi and melanomas can display similar morphologic changes during dermoscopic monitoring and may even grow at similar rates. Indeed, studies have demonstrated that nevi and melanomas removed during SDDI are often clinically and dermoscopically indistinguishable and that change alone permitted melanoma identification. However, the most relevant changes associated with melanoma during SDDI are asymmetric enlargement, appearance of focal or eccentric new structures (ie, “dermoscopic island”), or the appearance of atypical focal dermoscopic features such as vessels or regression features. Changing lesions with features concerning for melanoma should undergo biopsy, whereas lesions with equivocal features can undergo RCM or repeated dermoscopic imaging over a longer or sometimes indefinite time interval ( Fig. 5 ).
Related posts:
 Psoriasis Trends and Practice Gaps
Psoriasis Trends and Practice Gaps
 Practice Gaps and Training Gaps: Delineating What We Need to Fix
Clinical and Educational Gaps in Diagnosis of Nail Disorders
Practice and Educational Gaps in Dermatology
Practice and Educational Gaps in Surgery for Skin Cancer
Practice and Educational Gaps in Cosmetic Dermatologic Surgery
Practice Gaps and Training Gaps: Delineating What We Need to Fix
Clinical and Educational Gaps in Diagnosis of Nail Disorders
Practice and Educational Gaps in Dermatology
Practice and Educational Gaps in Surgery for Skin Cancer
Practice and Educational Gaps in Cosmetic Dermatologic Surgery
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


