49 Postoperative Care and Instructions
Summary
Keywords: wound care graft dislodgement crusting concealment pain swelling graft shedding
Key Points
•Daily hair wash instructions must be followed.
•How to avoid graft dislodgement.
•Expect transplanted grafts to shed.
•Be prepared for postoperative shock loss.
•Assure patients that adequate pain control will be addressed.
•Side effects are rare but should be reviewed.
49.1 Introduction
Many patients have significant anxiety postoperatively about damaging grafts, poor growth, and the healing process. Both clear postoperative instructions and an explanation of what to expect during the post-op period are important.
Common concerns that lead to anxiety and office calls include patients’ desire to understand how to handle postoperative scabbing, redness, itching, numbness, pain, and folliculitis. In addition, graft shedding, shock loss of native hair, and concern over the rate of hair regrowth also trigger many phone calls. These issues are discussed in the following sections, as well as in Chapters 50, 51, and 73.
We use both a post-op instruction handout and video to educate patients (Appendix 49.A; Video 49.1 and Video 49.2. We have found repetition and ample time to digest the information is helpful, so we mail the handouts out before surgery. We also review these materials at the end of surgery and again the morning after surgery during the patient’s postoperative hair wash, answering any questions they may have. The video is available on YouTube to view as much as needed.
We also give all patients a second handout that focuses more on what to expect with regard to the timeline of graft growth, and the way the recipient area will look at different stages postoperatively (Appendix 49 B). The more patients understand these issue, the smoother the postoperative course, for both the patient and the physician.
49.1.1 Typical Course of Graft Growth
•Patients often ask, “When are the grafts not at risk of falling out?” Bernstein and Rassman did a study indicating that grafts were safe by about 8 to 9 days.1
•Graft hair typically sheds between 2 and 6 weeks postoperatively and begin to regrow at 3 to 4 months. When growth begins, the hair is typically short, fine, and have minimal aesthetic effect. Usually by 6 to 7 months, enough caliber and length have developed to give 60 to 70% of the expected final cosmetic effect. However, it can take a full 12 months (an in some cases longer) to see the full aesthetic effect.
•Less commonly, transplanted grafts do not shed, but remain inactive for 2 to 4 months and then resume growth.
It is the editor’s observation that lack of shedding and early regrowth seems to be occurring more often recently. Perhaps this is due to technical improvements such as better holding solution or the use of implanters for placing. Although one could assume this would be associated with improved final growth, there are no studies as of yet that show this to be true.
49.2 Shampooing and Wound Care
49.2.1 Bandaging and Dressings
One of the older tenets of standard wound care is to keep the surgical area moist and clean, typically using an occlusive dressing.2 However, in modern hair transplantation, dressings are seldom used except in special situations when bleeding is unusually high. The tiny recipient sites heal well with simple cleaning and the application of wet compresses or sprays. The same is true for the donor area. The occasional need for dressing with excessive bleeding is discussed later in this chapter.
49.2.2 Recipient Site Shampooing
The first few days after surgery, blood and serum can ooze from around the grafts and cause a straw-colored or dark crust, which can stick to the grafts (Fig. 49.1). It is important for patients to shampoo and apply the recommended sprays or compress daily to prevent a large buildup of crust forming. We instruct patients to clean and shampoo the recipient area in the following way:
•Day 1: We recommend patients to return to the clinic the morning after surgery for their first shampoo. This allows you to demonstrate how to wash properly as well as examine the scalp for any issues that may have developed overnight (loose grafts, loose stitch, etc.).
•Week 1: Shampooing is done daily. During the first week, the patient should not use direct water pressure from the shower head. It can be too strong and cause grafts to become dislodged. Instead lukewarm water should be gently “poured” over the recipient site. We recommend using a large plastic cup (not glass). After wetting the scalp, shampoo should be lathered between the hands, gently patted onto the grafts, and left there for about 15 to 30 seconds. Afterward, the area can again be rinsed by pouring the lukewarm water over the hair. The epithelia tissue of the graft can absorb water during the shampoo and look like white bumps (Fig. 49.2). When patients see this, they often think something is wrong, and they should be assured it is completely normal. The grafts can be left to air dry or gently patted with a towel.
•Week 2: In the second postoperative week, patients may start to use the shower head with a gentle stream and the grafts can be gently massaged with lathered shampoo using the tips of the fingers. We tell them the goal is not to “scrub the crusts off” but rather to have the massaging motion loosen the scabs, so the gentle but steady flow of water running over them will wash them away. There is a yin and yang to shampooing: not too hard as to dislodge grafts, yet not too soft as to allow a large buildup of scabs.
•Week 3: After 2 weeks, the patient can return to a regular shampoo routine. Most commercially available shampoos are safe to use except medicated shampoos.

Fig. 49.1 Liposomal adenosine triphosphate (ATP) spray. Ten milliliter of liposomal ATP is added to 90 mL of normal saline to make a 10% concentration.

Fig. 49.2 Coagulated serum on the first post-op day. If the patient does not follow the daily shampoo directions, this could thicken and accumulate around the grafts.
Most clinics also have patients use a postoperative spray or wet compress to keep the recipient sites moist, prevent crusting, and promote graft survival. The sprays used vary from simple saline to more complex solutions like GraftCyte, which contain copper peptide and may promote healing.3,4,5
Recently, liposomal adenosine triphosphate (ATP) solutions have become popular as a post-op spray. After transplantation, revascularization of grafts does not start until day 3. During this period, the only way grafts get oxygen is by passive perfusion from the plasma (Table 49.1). There is evidence that delivering ATP to the cells during this phase decreases the effects of hypoxia and yields better growth (Fig. 49.3).6

Fig. 49.3 White epithelial tissue (red circle). When patients see this the first few post-op days, they think something went wrong with the surgery.
Table 49.1 Phases or revascularization
Stage 1 | Plasmatic imbibition | 1–3 d post-op, during which the graft absorbs plasma from the recipient site |
Stage 2 | Primary inosculation | 3–7 d post-op, during which early revascularization occurs and connections between the hair graft and recipient site |
Stage 3 | Secondary inosculation | Day 7, during which there are future changes in the blood vessels with coiled vessels extending deeply into the dermal papilla and with budding around the follicular implant |
49.2.3 Donor Area Shampoo and Wound Care
Caring for the donor area is less complicated as there are no grafts to worry about. The patient is simply instructed to wash the donor area with enough pressure to keep it clean and crust free. With staples, it is less painful to wash with an up-and-down motion, which prevents the fingers bouncing over the staples. With sutures, patients need to be careful when using a comb to avoid the teeth getting caught under a stitch.
Many clinics have the patient apply an ointment to the donor site after washing to maintain hydration and a barrier to bacteria. Bacitracin, Neosporin, and mupirocin are popular antibacterial ointments used. Neosporin is associated with contact dermatitis, and therefore not recommended. Some patients ask about “natural products” like vitamin E (or other natural oils). This is probably OK, but vitamin E oil has also been associated with contact dermatitis, and therefore should be used cautiously.3
49.3 Suture/Staple Removal
49.4 Dislodged Grafts
Sometimes a patient will call saying some of the grafts have come out. Usually, this is due to accidental trauma. After surgery, their head is numb and their kinesthetic sense of where their head is in space is disrupted. Patients should be warned about this. If grafts become dislodged, they may be able to be reimplanted safely if they are immediately placed in a small cup of the postoperative spray provided to them, or alternatively into a cup of water with one-fourth teaspoon of salt, and not too much time has passed.
49.5 Postoperative Medical Complaints
49.5.1 Pain
Pain is usually mild/moderate in most patient, requiring only Tylenol or nonsteroidal anti-inflammatory drugs (NSAIDs). However, some patients have substantial pain, especially the first post-op night after the anesthesia wears off. These patients may need stronger pain medication and therefore we give patients a small supply of tramadol (~12 pills) to use if they need it. We try to time the surgery, so the patient is reinjected with long-acting Marcaine and still numb when they leave the office. We tell them to take an NSAID or possibly a tramadol when they get home so it is on board when the anesthesia wears off. We have used injectable Toradol (ketorolac) at the end of surgery for the same reason in patients we feel may have a low pain threshold.
49.5.2 Bleeding
It is common to have some bleeding or oozing from the donor site, especially the first night after surgery. Patients should be provided with disposable waterproof pillow cases or chucks to put over and protect their pillow. Patients should be told that it is normal to see some blood on the disposable pillowcase in the morning.
Sometimes the donor area is oozing a little more than expected after surgery. In this case, a temporary dressing can be applied to deliver some pressure until the bleeding stops. Typically, the bleeding stops quite quickly, and dressing can be removed in a few hours after the patient gets home. If bleeding persists, the patient should call for more instructions.
Occasionally, there is some oozing from the recipient site that needs to be controlled. The patient should be given gauze and told to place gentle pressure for 2 minutes, which usually stops the bleeding.
49.5.3 Edema
Edema of the forehead can occur after surgery. This should not be a surprise when one considers the thousands of tiny incisions and tumescent solution placed in the scalp.
If edema does occur, it usually starts on post-op day 3, will peak on day 4, and be gone by post-op day 5 or 6. There are a few measures that can be done to significantly minimize or prevent the occurrence of edema:
•Having the patient sleep with their head above their heart (a 20- to 30-degree angle) for the first 2 days after surgery.
•Applying a cold pack to the forehead for 10 minutes four times a day.
•Massaging forehead edema from the midline laterally to the temporal point area helps drain the lymph system.
•Corticosteroids: The Abassi study suggests that the use of steroids is the most effective of all measure to reduce edema. His study also suggested that adding corticosteroids to the tumescence solution was superior to oral or intramuscular steroids (Table 49.2).7
Table 49.2 Steroids medication and dosage
Route | Medication | Dosing |
Oral | Prednisone | 40–60 mg on the day of surgery. Either in one dose or divided doses. Continue for 5 d |
Intramuscular (IM) | Celestone Soluspan | 1 to 2 mL IM on the morning of surgery |
Added to tumescence | Normal saline >100 mL Epinephrine 1/1,000, 1 mL + triamcinolone acetate, 40 mg | Added to scalp and donor site as needed to raise skin |
If these measures are taken, edema is usually avoided or minimal, but if it does occur, the patients can be assured it will resolve by 7 days and not affect survival.
49.5.4 Hiccups
Hiccups are an infrequent but bothersome post-op sequela. Most feel hiccups are due to the administration of diazepam or steroids during surgery as both have been shown to cause hiccups. Another cause may be irritation of the sensory branch of the phrenic nerve (located in the posterior auricular area) during strip surgery. If nothing is done, they can last from a few hours to a few days. Many home remedies and physical maneuvers can resolve this condition. However, persistent hiccups are best treated with chlorpromazine 25 mg orally every 4 to 6 hours until the hiccups resolve (Table 49.3).8
Table 49.3 Treatment of hiccups
Physical maneuvers | Breath holding, Valsalva maneuver, breathing into bag, ice water gargles, swallowing granulated sugar, drinking from opposite side of glass, biting on a lemon, fright, noxious odors (inhaling ammonia), pressing on the eyeballs, pulling knees to chest or leaning forward to compress chest |
Physical maneuvers done by the physician | Catheter or cotton swab stimulation of the naso-oropharynx, forcible traction of tongue, phrenic nerve message |
Drug therapy | Antipsychotics (chlorpromazine, haloperidol), anticonvulsants (phenytoin, valproic acid, carbamazepine, gabapentin), muscle relaxants (baclofen, cyclobenzaprine) |
49.5.5 Itching/Pruritus
Itching can occur in the recipient area after a transplant. The cause may be dry scalp or the normal healing process. The physicians should stop minoxidil if it is being used and look for other causes of contact dermatitis. It usually resolves by itself but cool sprays, or cold packs, can give some relief. If needed, patients can use antihistamines or topical corticosteroids for relief.
49.6 General Concerns
49.6.1 Exercise
Patients should take it easy the first week after surgery to promote healing and limit the risks of accidental trauma. For the recipient area in both follicular unit excision (FUE) and follicular unit transplantation (FUT), after 1 week the skin surface has sealed, so exercise should not affect graft survival. We still tell patients to avoid activities where they could hit their heads for a few weeks (e.g., skiing, soccer, etc.).
With strip-FUT, the donor wound is susceptible to stretching for a few months post-op, so we tell patients to avoid activities that put excessive force on the occipital area during this time.
With FUE, the donor area heals as quickly as the recipient area and there are really no restrictions after 1 week.
49.6.2 Returning to Work
The two factors that determine when a patient can go back to work are the physical demands and the desire for privacy.
Physical Demands
If a patient has a job with no physical demands, they theoretically could go back the next day and it will not affect the results of surgery. On the other hand, if a patient has a physically demanding job where there is strenuous activity and possibly the risk of graft trauma, it is probably best they take off work for 7 to 10 days.
Privacy Concerns
Many patients want to hide the fact that they had a hair transplant from friends and coworkers. This will limit their ability to return to work and engage in other social activities until they feel comfortable.
In most cases, the actual signs of surgery such as visible recipient sites, crusting, and redness are gone by 7 to 10 days. Often, it is the abnormal haircut done at the time of surgery, rather than the visible grafts, that draws attention to the patient. The ability to conceal the procedure varies depending on multiple factors including the recipient site location, amount of preexisting hair, extent of recipient/donor site shaving, and type of procedure performed (FUE vs. FUT).
If the patient can wear a hat to work, concealing the transplant will not be an issue. But many patients cannot wear hats to work.
In smaller FUT procedures, a transplant can be hidden almost immediately if grafts were placed within preexisting hair and no major shaving of the recipient site was done or if the preexisting hair is long enough to cover the transplanted area with some creative styling (Fig. 49.4 and Fig. 49.5).
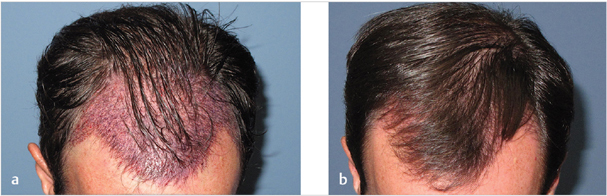
Fig. 49.4 Frontal two-thirds transplanted without cutting hair. (a) Day after surgery, the transplant is still visible. (b) Four days post-op. It is easy to conceal the transplant with the patient’s existing hair.
Related posts:
 Hair Anatomy and Histology for the Hair Transplant Surgeon
Hair Anatomy and Histology for the Hair Transplant Surgeon
 Plugged in: How to Ensure That Your Practice Thrives (and Survives) in Today’s DigitalWorld
Plugged in: How to Ensure That Your Practice Thrives (and Survives) in Today’s DigitalWorld
 Transplanting into Areas of Cicatricial Alopecia
Transplanting into Areas of Cicatricial Alopecia
 Special Considerations for Postoperative Care in Follicular Unit Excision
Special Considerations for Postoperative Care in Follicular Unit Excision
 Hairline and Recipient Area Repair of Poor Previous Transplantation
Hairline and Recipient Area Repair of Poor Previous Transplantation
 Ergonomics in Hair Restoration Surgery: FUE Technique
Ergonomics in Hair Restoration Surgery: FUE Technique
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


