Introduction
In the field of reconstructive surgery, not a day goes by without a skin flap being used. The earliest description of skin flaps was by Sushruta in 600 bc and this was, in fact, a local flap, of axial type. The flap described by Tagliacozzi in 1597 was a random pattern flap from the medial aspect of the upper arm. These two flaps, being a local flap and distant flap, respectively, were both used for reconstruction of the nose. Despite extensive studies of the blood supply to the skin by Manchot in 1889 and Salmon in 1936, most of the reconstructions during the First and Second World Wars were by tube pedicles. In 1973, McGregor and Morgan classified skin flaps into axial and random pattern flaps. Ponten highlighted the value of fascia in augmenting the blood supply to the skin. In 1995, Batchelor and Moss reported that the fascia acts like a scaffold for the sub-, intra-, and suprafascial vascular plexus. Taylor and Palmer in 1987, proposed the concept of “angiosomes” (vascular territories) and choke vessels. With this knowledge, the floodgates were opened for various types of fasciocutaneous flaps.
The skin plays an important role in protecting the body and thermoregulation. It is separated from the underlying structures by connective tissue called fascia. The skin, in order to regulate the temperature of the body, needs a rich blood supply; hence there is a regular connection between the vessels within the tissue compartment and the skin via various perforations in the deep fascia. Taylor identified an average of 374 cutaneous perforators in the body. Fujino, in 1967, demonstrated the importance of perforators in the circulation of skin flaps. He also reported that the perforators and the axial vein are important for interstitial fluid turnover.
There are different types of perforators. Our own clinical observations have identified two distinct vessels: the perforating vessels, which penetrate the deep fascia and have an artery and venae comitantes, and the fascial feeder vessels, which do not penetrate the deep fascia but terminate under it. The latter are mainly arterial without any venae comitantes. Both the perforators and the fascial feeders take part in the formation of the subfascial, intrafascial, and suprafascial plexi. These in turn communicate and form a rich plexus under the skin.
We now have various types of skin flaps based on perforating vessels and this has led to some confusion. To alleviate this, Wei et al. in 2001 defined perforators as those vessels that penetrate muscle on their path toward skin. But, anatomically, the blood vessels that supply the muscles, bone, and large tendons also penetrate the deep fascia to supply the skin. In addition to these vessels, there are blood vessels called “septocutaneous direct perforators” that also perforate the deep fascia and these travel between muscles and compartments. Linton published a detailed study of the septocutaneous vessels of the leg and used the term “perforator”. He described the communicating veins between the superficial and deep systems and the accompanying artery. In 2009, Saint-Cyr et al. introduced the term “perforasome.” Each perforator holds a unique vascular territory and by direct and indirect linking vessels they form a network and play a critical part in perforator flap perfusion.
Numerous anatomic cadaveric studies have established the number, location, and type of perforators of the posterior tibial artery. For practical purposes, the leg has been divided in many ways: into an upper concealed part and a lowed exposed part ; into five 7 cm parts ; into four zones ; three zones ; and 10 equal parts . Most recently, Shaverian and Saint-Cyr found that there were three constant clusters of perforators at 4–9 cm, 13–18 cm, and 21–26 cm from the medial malleollus.
There are a greater number of longer and larger-caliber, muscle-type perforators in the upper half, while the perforators of the lower half, or lower third, of the leg are the shorter, direct cutaneous type. My own clinical observation is that there are three direct septocutaneous perforators in the lower third, which correspond to Linton’s venous connection between the superficial and deep vein system. These perforators communicate with each other as well as with the anterior tibial and perineal artery perforators, to form a suprafascial level network.
There is also a rich vascular network forming a circle of anastomoses around the ankle joint. This knowledge will help reconstructive surgeons to use various perforating flaps based proximally or distally around the knee and ankle joints ( Table 61.1 ).
| Anatomic Study | Zone | Number | Caliber (mm) | Pedicle length (cm) | Location from medial malleolus (cm) | Clusters |
|---|---|---|---|---|---|---|
| Carriquiry et al. (1985) | 3 | 4–5 | 0.5–1.5 | – | 9–12 17–19 22–24 | – |
| Liu et al. (1990) | 2 | – | – | – | – | – |
| Koshima et al. 1992) | 5 (7 cm) | 3.1 ± 0.8 | – | – | – | – |
| Wu et al. (1993) | 4 | 2–5 | 1.0–1.5 | – | 8–15 | Zone II |
| Hung et al. (1996) | – | 5–8 | 1.5 ± 0.2 | 4 ± 1.3 | 18.6 ± 4.5 | – |
| Whetzel et al. (1997) | 10 | 3–8 | 0.5–1.0 | – | – | 95% in lower |
| Taylor and Pan (1998) | Anterior Posterior | (SC) 6–16 (M) 1.5 (SC) 2.5 | 0.76 1.15 | – | – | – |
| Ozdemir et al (2006) | 3 | – | 0.4–2.1 0.5–2.0 0.3–1.5 | – | Upper third Middle third Lower third | – |
| Shaverian and Saint-Cyr (2008) | 3 | 4.9 ± 1.7 | 1.0–1.5 | – | 4–8 13–17+21–25 | – |
| Tang et al. (2009) | – | 4–9 | 0.6–1.2 | – | – | Lower-half septocutaneous Upper-half muscle-cutaneous |
The posterior tibial artery perforator has septocutaneous, musculocutaneous, and periosteocutaneous perforators as described by Koshima et al. in 1992. We also noticed that, apart from these perforators, there are vessels that supply the Achilles tendon and also perforate to supply the skin. These are called “tendinocutaneous.” Based on these perforating vessels, it is possible to raise small cutaneous flaps as local flaps to cover the exposed bone and tendon over the leg.
The perforator concept has become a method of choice in reconstruction both as free and local pedicle flap. This requires two basic understandings: the knowledge of blood supply of the skin and the surface anatomy of muscles and compartments. This will help in locating perforators and planning a flap for reconstruction.
A Doppler is a useful tool to use prior to raising perforator flaps, especially pedicled perforator flaps. CT angiography is a useful but not essential form of imaging, as most perforator-based flaps do not require intramuscular dissection.
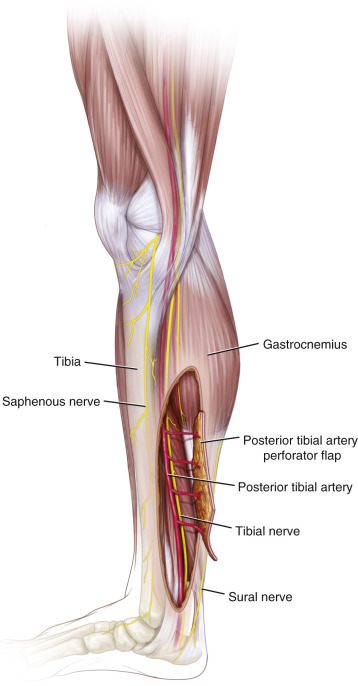
Flap Anatomy ( Fig. 61.1 and see Ch. 13 and Fig 13.6 , Fig 13.7 , Fig 13.10 , Fig 13.11 , Fig 13.12 , Fig 13.13 , Fig 13.19 )
The fasciocutaneous or adipofascial flaps, based on perforating vessels of the posterior tibial artery, can be proximally or distally based. For defects over the foot, reverse posterior tibial artery flaps can be used, incorporating all the perforators of the posterior tibial artery.
Arterial Supply of the Flap ( Fig. 61.1 and see Figs 13.6 and 13.10 )
Dominant:
perforators from posterior tibial artery
Length: 4 cm (range 2–6 cm)
Diameter: 1.5 mm (range 1–2 mm)
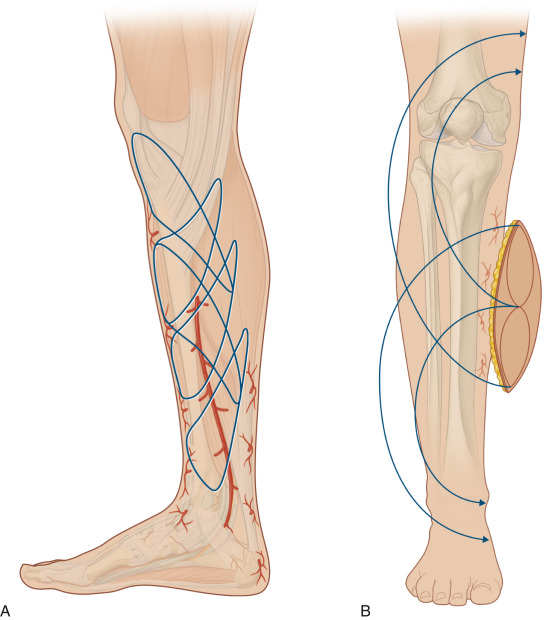
Perforators form three perforating vessels on the medial side of the leg, which can be located between 9–12 cm, 17–19 cm, and 22–24 cm from the tip of the medial malleolus.
Septocutaneous vessels, which are the direct link between the main vascular trunk and the fascia and skin, supply this flap. The perforators can be traced to the posterior tibial artery, which can be included with the flap to increase the pivot point. In that case, the vessel length could reach proximally up to the knee joint and distally to the foot.
It is not wise to sacrifice the major vessel of the leg. Only in exceptional situations, where all the three vessels of the leg are intact and when there are no other options available, is the local option of using the posterior tibial artery perforator flap possible.
Minor:
random pattern supply from the plexus of the fascia
The plexus of vessels in the fascia is fed not only by perforators but also by fascial feeder vessels (Ponten superflap). The fascial feeders are inconsistent and are only very fine arterial vessels with no accompanying veins.
Venous Drainage of the Flap (see Fig. 13.19 )
Primary:
venae comitantes of the perforator artery
Length: 4 cm (range 2–6 cm)
Diameter: 0.75 mm (range 0.5–1 mm)
Secondary:
cutaneous veins draining into long saphenous or short saphenous system (Fig. 13.20)
The secondary vein is included in the flap only when there is inadequate venous drainage (long and short saphenous veins).
Flap Innervation (see Fig. 61.1 and Fig. 13.19 )
Sensory:
The cutaneous nerve on the anteromedial aspect of the leg is the long saphenous nerve. Similarly, branches of the sural nerve supply the posterior aspect of the leg.
Motor:
This flap can contain a small segment of muscle that would receive its blood supply in a reverse manner; however, the segment of muscle would not be transferred as a functional muscle unit.
Flap Components
The flaps based on perforators of the posterior tibial artery are mostly fasciocutaneous or adipofascial type. As the perforators of the posterior artery anastomose with other perforators, it is possible to incorporate a small amount of muscle, bone, and tendon. These structures are transported in part with the flap and this part is vascularized by the flap in a reverse manner.
Advantages
- •
The posterior tibial artery skin flap is ideal for small defects in the leg, to reconstruct exposed bone and tendon. As it is local tissue, it replaces like tissue.
- •
Harvesting the flap requires a shorter operating time and hence, the flap is ideal for patients who are not fit for a lengthy procedure.
- •
The posterior tibial artery perforator flaps have also been used as regional flaps and as free flaps. Koshima and Soeda have used perforator posterior tibial flaps without sacrificing the main vessels.
- •
The flap is relatively thin and can be used to resurface defects in regions such as the hand and fingers requiring thin tissue.
- •
Most of the perforators are septocutaneous, therefore simplifying the dissection.
- •
The flap can include soleus muscle or a segment of tibia bone.
Disadvantages
- •
The main disadvantage in a skin-grafted donor site is when a large cutaneous flap has been either proximally or distally based. This leaves an unsatisfactory donor site scar. This can be avoided by using a propeller flap or V-Y advancement flap.
- •
Loss of sensation distal to the flap as the cutaneous nerve is included in the flap.
- •
Limited pedicle length when the flap is based on the perforators only. This can be alleviated by including the posterior tibial artery with the flap.
Preoperative Preparation
In this section the reconstructive surgeon should consider three factors: the patient, the wound, and the leg.
Assess the patient regarding fitness for surgery, age (posterior artery perforator flaps can be used with any age), and sex (one has to bear in mind the resulting donor site morbidity, especially in young female patients). Assess other medical conditions, i.e., diabetes mellitus, arteriosclerosis, and conditions such as pyoderma gangrenosum. Take the necessary steps to optimize the patient’s medical condition prior to surgery.
The wound should be assessed as to whether it is clean with healthy granulation tissue and for the presence of infection, while exposure of underlying structures such as bone and tendons should also be assessed. The extent of disease process or traumatized field surrounding the wound should be assessed. An absolute contraindication to a perforator flap is a degloving injury, as generally, the perforators are severed. Relative contraindications include patients who are obese, diabetic, chronic smokers, and sufferers of pyoderma gangrenosum.
The vascularity of the leg should be assessed before the operation by the presence of peripheral pulsations of the three major vessels of the leg. An arteriogram is helpful but not essential. In approximately 6% of patients, the posterior tibial artery is weak or absent.
Before the operation, the leg is shaved and cleaned with antiseptic solution. Prophylaxis against deep vein thrombosis is given perioperatively.
Flap Design
Anatomic Landmarks ( Figs 61.2 , 61.3 )
The donor area of the posterior tibial artery perforators extends anteriorly to the anterior border of the tibia and posteriorly to the midline of the posterior aspect of the leg. All the perforators of the posterior tibial artery perforate the deep fascia in a longitudinal line from the tibial tuberosity superiorly to the medial malleolus inferiorly.
General Thoughts About Flap Design
Knowledge of the vascularity, distribution, and location of the perforators helps the operating surgeon to design a flap based on posterior tibial artery perforators. It is possible to design flaps such as large rotation, propeller, and V-Y advancement flaps to avoid unsightly donor site skin grafts. When a V-Y flap is used, it should be in the oblique axis, keeping the tail of the V-Y toward the calf, as there is usually extra skin for direct closure. If it is not possible to close the donor site, it can be grafted with split skin temporarily.
The reach of the flap can be extended by placing the perforator in an eccentric position when designing the flap.
The flap should be designed based on the more distally located perforators, since many of the proximal perforators are musculocutaneous and require an intramuscular dissection if the flap is to be advanced significantly or used as a free flap.
Special Considerations
Small defects over the distal part of the leg can be reconstructed by a V-Y advancement flap. However, larger defects with exposed bones will require either a propeller or a transposition flap. When local options are not available, one should think about free tissue transfer.
Always consider the age, sex, and general condition of the patient first. Next, consider the vascularity of the leg and lastly the type of wound that requires reconstruction.
Differences in Design, if Any, When Performing the Flap as Pedicled or Free
The pedicled flap design depends entirely on the site of the wound. For practical purposes, the leg is divided into upper, middle, and lower thirds ( Fig. 61.2 ).