Chapter 43 Table 43.1 Posterior interosseous flap (reverse pedicled flap)
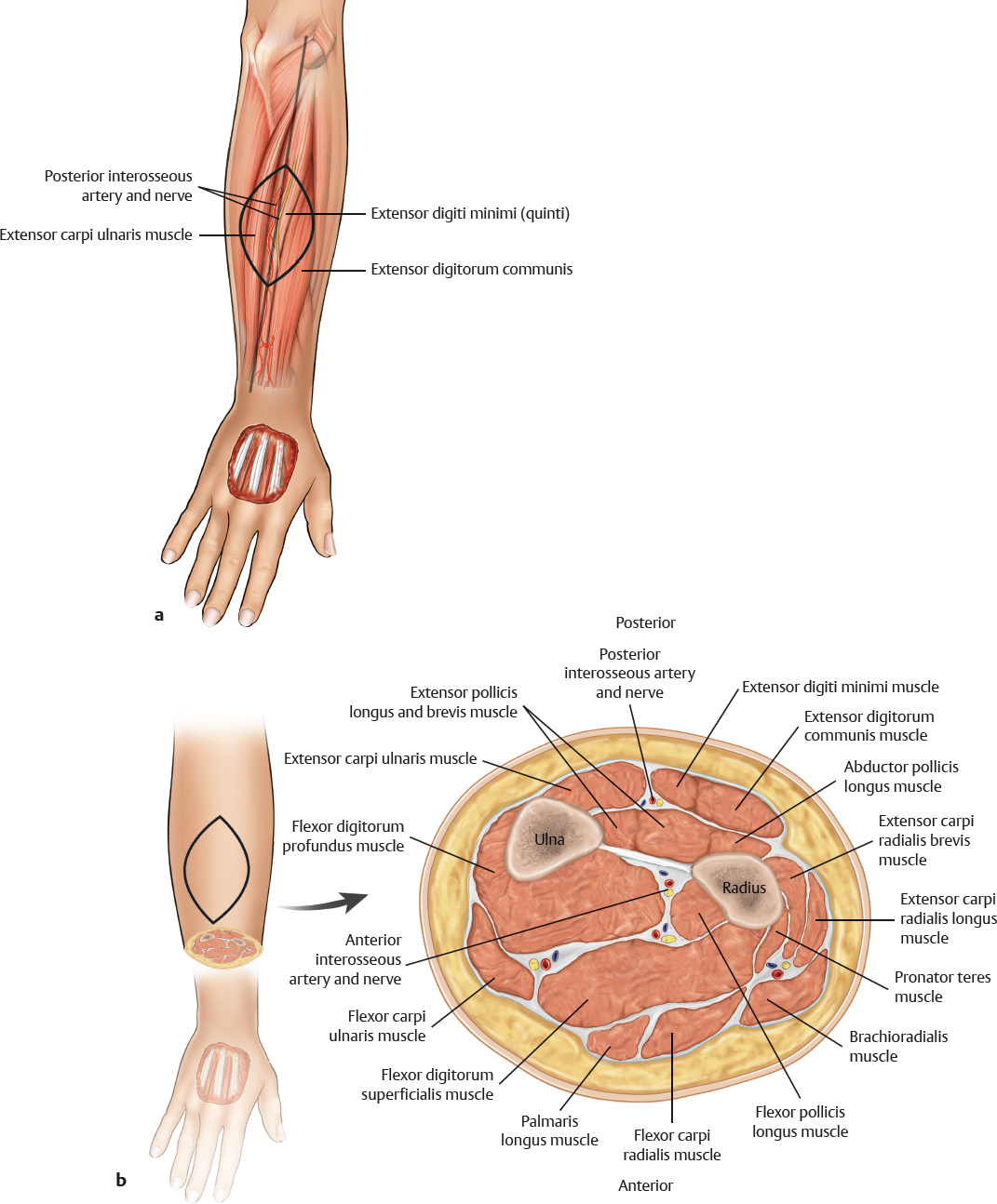
Posterior Interosseous Flap
Table 43.2 Posterior interosseous flap (free flap and antegrade pedicled flap)
Flap |
|
Tissue | Skin and fascia |
Course of the vessels | Deep to the flap surface in a fascial septum; antegrade vessels in the free flap |
Dimensions | 8 × 15 cm; donor sites of flaps < 4 cm wide can be closed primarily |
Extensions and combinations | Tendon strip from the extensor carpi ulnaris; bony segments from the radius |
Anatomy |
|
Neurovascular pedicle | — |
Artery | Posterior interosseous artery; antegrade vessel from the radial artery |
Veins | Venae comitantes |
Length and arc of rotation | Pedicle length, 3–4 cm |
Diameter | Artery, 2–3 mm; vein, 2.5–3.5 mm |
Nerve | Ulnar cutaneous antebrachial branch |
Surgical technique |
|
Preoperative examination and markings | Draw a line from the lateral epicondyle to the dorsal center of the wrist; perform a Doppler examination of the two main perforators at the proximal third of the forearm; outline the flap and center it over this line |
Patient position | Supine with arm on arm table |
Dissection | Incise laterally along the marking; incise the muscle fascia; perform a subfascial dissection until the fascial septum between the extensor digiti quinti and the extensor carpi ulnaris can be identified; create a medial incision; perform a subfascial dissection until the septum is identified from the other side; free the septum from the periosteum in a distally cephalad direction; ligate the pedicle distally; raise the flap until the pedicle branches off toward the radial artery; watch out for nerve branches supplying wrist extensors; open the tourniquet; check for adequate perfusion; rotate the flap or ligate the pedicle and then inset the flap in the recipient site |
Advantages |
|
Vascular pedicle | Adequate caliber |
Flap size and shape | Donor sites of flaps < 4 cm wide can be closed primarily; subcutaneous fat can provide excellent gliding tissue for tendon reconstructions |
Combinations | Inclusion of tendon strip and bone segments enhances versatility |
Disadvantages |
|
Pedicle | Pedicle is short; nerve transection may be required if motor branches cross between main perforators |
Bulkiness | Can be bulky in strong patients with fleshy forearms |
Donor site morbidity | Donor site can be very conspicuous; this flap should not be the first choice for younger patients and females |
Pearls and pitfalls |
|
Dissection | Try to spare the motor nerve; avoid a too narrow arc of rotation, because the flap has a tendency for venous congestion; include a proximal subcutaneous vein for emergency turbocharging; include a wide segment of dorsal fascia with the pedicle; identify the arterial anastomosis to the anterior interosseous artery first (5% of all patients do not have this anastomosis) |
Extensions and combinations | Include a tendon strip in the subfascial dissection; stay very close to the periosteum to avoid injury to the pedicle |
Contouring and correction | Secondary corrections may be required in many cases |
Clinical applications | Forearm defects; dorsal hand defects; complex reconstructions with free nonvascularized tendon grafts; defects around the elbow when used as proximal pedicle flaps |