brown macules noted on the lips, mucosal surfaces, and genitalia, should alert the clinician for potential Peutz-Jeghers syndrome (Figure 7-6). Patients diagnosed with this syndrome during childhood are at higher risk for gastrointestinal adenocarcinomas and breast and ovarian cancers.
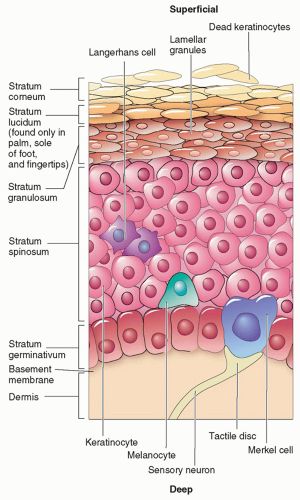 FIG. 7-1. Anatomy of the epidermis and location of melanocytes. |
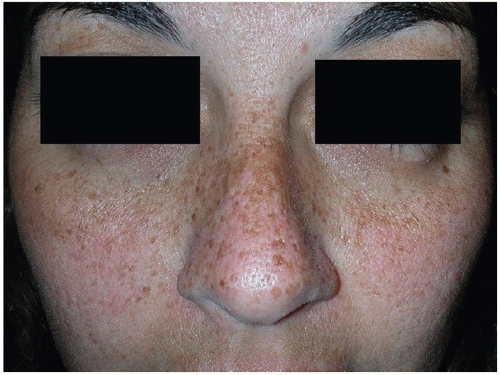 FIG. 7-2. Ephelides or common freckles are the result of UVR exposure and usually fade in the winter. |
 FIG. 7-3. Lentigo simplex. |
 FIG. 7-4. Solar lentigines from sun exposure do not fade in the winter. Noted “ugly duckling” lesion upon examination. |
respectively). A full skin examination should be performed to assess for the number and size of café au lait macules/patches, presence of neurofibromas and axillary freckling. Patients with clinical presentation suspicious for NF1 or NF2 should be referred for neurologic and developmental evaluation (see chapter 6). In adults, a full skin examination should be performed for skin cancer screening.
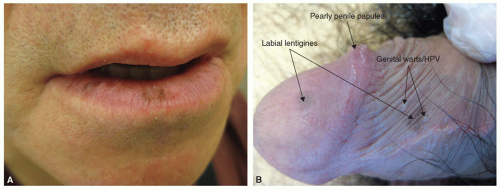 FIG. 7-5. A: Labial lentigines more common on the lower lip. B: Penile lentigines in addition to pearly penile papules and HPV. |
 FIG. 7-6. Orolabial lentigines suspicious for Peutz-Jeghers syndrome. |
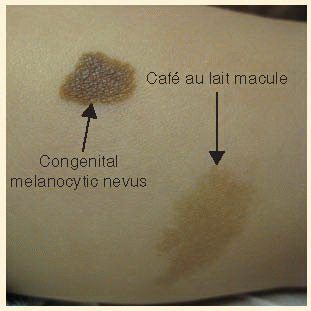
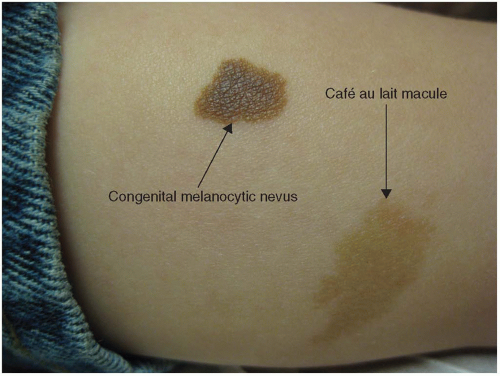 FIG. 7-7. Comparison of a café au lait macule beside a small congenital melanocytic nevus. |
keratinocytes, hair follicles and melanoctyes. They are usually unilateral and may be associated with ipsilateral hypoplasia of breast and skeletal anomalies, including scoliosis, spina bifida occulta, or ipsilateral hypoplasia of a limb (Figure 7-9).
 FIG. 7-8. Nevus spilus. |
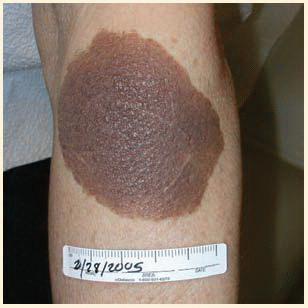
 FIG. 7-9. Becker’s nevus classic presentation on the shoulder or upper chest. |
 FIG. 7-10. Dermal melanocytosis or common Mongolian spot commonly located over the sacrum. |
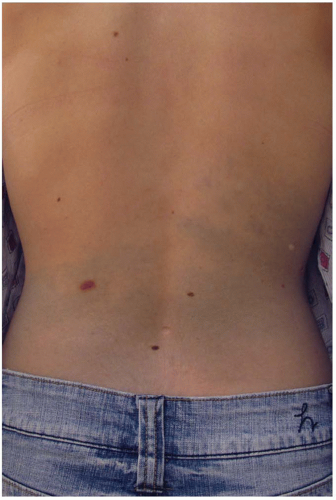 FIG. 7-11. Less common dermal melanocytosis in a Caucasian adult. |
Like any pigmented lesion, these should be monitored for signs and symptoms of melanoma. Glaucoma has been associated with nevus of Ota. Although usually benign, these lesions can have a psychological impact on the patient’s body image. Camouflage makeup is often used, but topicals have no effect. Q-switched laser, requiring repeated treatments, provides the most promising cosmetic results.
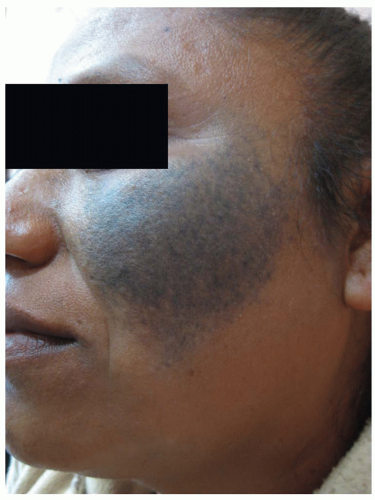 FIG. 7-12. Nevus of Ota. |
Location: Single digit, thumb, or great toe nails
Appearance: Fast growth, longitudinal melanonychia, band width more than 3-5 mm
Hutchinson’s Sign: Periungual pigmentation of skin
Nail Dystrophy: Notch in free distal nail margin, surface irregularity, oozing, or bleeding lesion similar to ingrown nail
 FIG. 7-13. A: Child with medium-sized CMN on the lip and chin of infant with significant cosmetic impact. B: Medium CMN. |
Congenital: present at birth or soon thereafter
Acquired: occurs after 6 months old
Epidermal: arising in the epidermis only
Junctional: arising at the dermal-epidermal junction
Dermal: nests in the dermis or subcutaneous fat only
Compound: a combination of junctional and dermal
Melanocytic: melanocytes only
Spindle cell: spindle-shaped cells as in Spitz nevus
Blue pigmented cells: Cellular blue nevi
Lesions characteristics were added to the classification system as variables influencing risk for malignancy (Box 7-3). The stratification of CMN sizes was also expanded to include a separate “giant size” category. Large CMN overlying the spinal column and skull have been associated with neurocutaneous melanocytosis (NCM) with symptoms of increased cranial pressure, vascular birthmarks, spinal cord compression, tethered spinal cord, or leptomeningeal melanoma.
TABLE 7-1 Risk Stratification Based on Size of Congenital Melanocytic Nevi | |||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| |||||||||||||||||

|
Related posts:



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


