The perforator-plus flap is a new concept for lower extremity reconstruction. It combines a perforator flap with a traditional skin rotation flap. It can be another option for lower extremity soft tissue defects since the flap has an augmented blood supply. The ability to detect cutaneous perforators has improved with the Duplex scan imaging technique. These advances have made the perforator-plus flap a viable option for soft tissue reconstruction. It can be versatile and reduces donor site morbidity; it is technically simple to perform and faster than traditional free flaps. It achieves durable soft tissue coverage for lower extremity wounds.
Key points
- •
The perforator-plus flap combines a perforator flap with a traditional skin rotation flap.
- •
Ubiquitous use of hand-held Doppler and other preoperative imaging techniques make the perforator-plus flap a viable option for soft tissue reconstruction.
- •
The flap is technically simple to perform and faster than traditional free flaps.
- •
It is a viable alternative option for soft tissue reconstruction once targeted perforators are identified.
Introduction
Lower extremity trauma remains a reconstructive challenge to plastic surgeons. Many such defects occur as a result of high-energy impact and are often associated with concomitant osseous and vascular injuries. The treatment concepts for traumatized lower extremities have evolved throughout modern times, with the most contemporary advances in the field of microsurgery. This has led to reliable use of free tissue transfer for coverage of the distal third of leg wounds, with current literature in agreement with this treatment algorithm. ,
Even though free flaps are a readily available option for lower extremity soft tissue coverage, they may not be the best solution in every patient because of donor site morbidity and the surgeon’s access and expertise to microvascular free tissue transfer. Research in the angiosome and perforasome concepts have introduced another reconstructive solution: the perforator flap. However, classic perforator flaps are restricted by their sole vascular pedicle, which can limit the flap design because of concern over inadequate circulation, especially venous congestion and ultimate success of flap coverage.
The perforator-plus flap can be considered a modification of the classic perforator-based fasciocutaneous flap. Instead of the skin paddle being supplied solely on the isolated perforator, the perforator-plus flap allows for an augmentation of the vascular supply to the perforating pedicle by keeping the skin paddle attached to a cutaneous base. Both the arterial inflow and venous outflow become more reliable. In exchange for a smaller arc of rotation, a larger and more robust skin flap can be designed. Although this flap does not replace free tissue transfer, it does offer reliable soft tissue coverage in appropriate wounds, with the added benefit of sparing the patient additional donor site complications and prolonged operating time. Additionally, it does not exclude from higher level of microvascular reconstruction.
Indications and contraindications
The indications for perforator-plus flaps are the same as for any local or regional flaps as long as reliable perforators within the flap territory can be reliably identified and the flap itself is not within zone of injury. The common indications for perforator-plus flaps in the senior author’s practice are any less extensive lower extremity soft tissue defects with exposed hardware or vital structures. This could be any acute or chronic wounds (up to 50 cm 2 ) in the lower extremity, but the timing of such a reconstruction depends on zone of injury and mechanism of injury. In general, definitive flap reconstruction is usually performed within 7 to 10 days after injury in the acute setting if the patient’s medical condition is permissible.
The contraindications are poor local soft tissue compliance (ie, radiation changes, poorly controlled lymphedema); absolute limb salvage contraindications or patient desire for amputation; and no available local perforasomes secondary to zone of injury or prior surgery/scars; and large defects that require more soft tissue coverage than locally available flap tissue.
Preoperative evaluation and special considerations
The patient is seen in consultation and the wound evaluated. The surgeon must take into account the acuity of the wound, the zone of injury, defect size, and defect components. Additionally in the acute setting, one must consider evolving tissue loss. Unlike free-tissue transfer, the use of a local perforator-plus flap relies on a reliable local soft tissue donor site.
The authors prefer the use of intraoperative Duplex scan in addition to a hand-held Doppler to accurately identify target perforators. In general, at least 1 good perforator is needed for the design of such a flap. The ad hoc nature of this step can be considered free style, as it relies on the reconstructive surgeon’s expertise to determine the planned approach. However, preoperative CT angiogram may also serve as adjunct to presurgical workup. This does not replace intraoperative Duplex or Doppler to pinpoint the exact locations of the cutaneous perforators. Because there may be several adjacent perforators, the flap design is finalized based on the most appropriate perforator and arc of flap rotation to maintain a skin bridge prior to the start of the flap dissection.
Ultimately, it is important to evaluate the defect in light of the patient’s potential donor sites and the associated morbidity of free tissue transfer. However, if a perforator-plus flap is chosen as the first-line reconstructive option, it is imperative to discuss with the patient the step-wise approach of possible regional, distant, or free tissue transfer as salvage options.
Surgical procedures
Pertinent Anatomy of the Flap
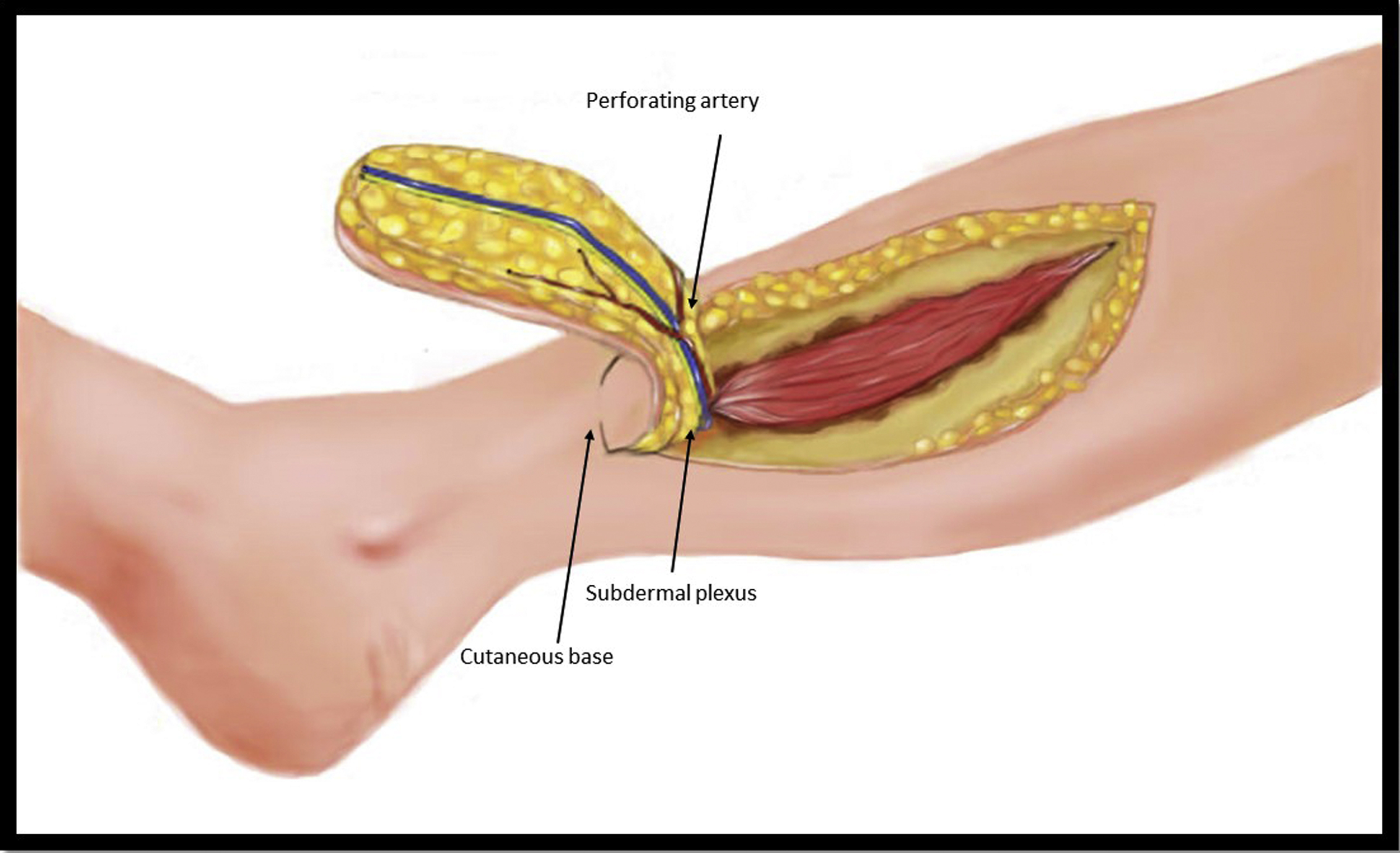
The perforator-plus flap receives its blood supply primarily from 1 or 2 or more musculocutaneous or septocutaneous perforators, the same as any other free style pedicled perforator flaps. It also receives an additional blood supply from the intact skin bridge, since both the arterial inflow and venous outflow can be augmented ( Fig. 1 ). Depend on the width of the skin bridge, the flap itself may even survive based on the intact skin connection. With this kind of flap design, the perforator-plus flap would be more reliable, since an additional skin bride can serve as a supercharge that can minimize ischemia or venous congestion of the flap. Therefore, in exchange for a smaller arc of rotation, a larger and more robust skin flap can be designed.
Flap Design and Dissection
The flap design is essentially the same as a skin rotation flap. The flap is marked with a marking pen first, and at least 1 perforator within the flap territory is then identified with a duplex scan ( Fig. 2 ). The information regarding the size, blood flow, and intramuscular course of each perforator can be obtained. All perforators are again confirmed by a hand-held Doppler before flap elevation. The incision is carried down to the level of the fascia, and a suprafascial dissection is completed to raise the skin paddle, keeping the most proximal portion attached to its cutaneous base. The width of such a skin connection really depends on the required arc of flap rotation ( Fig. 3 ). During the flap dissection, attention is paid to identify and preserve the perforators ( Fig. 4 ). Although intramuscular dissection of the perforator can be performed, it is usually not necessary, since the flap can be rotated and advanced to the defect without difficulty ( Fig. 5 ). If necessary, intramuscular dissection of the perforator can be performed to improve arc of the flap rotation. This can be facilitated by use of a hand-held Doppler. A skin graft is often needed for the flap donor site as any other skin rotation flaps ( Fig. 6 ).

Related posts:
 Propeller Flaps in Lower Extremity Reconstruction
Propeller Flaps in Lower Extremity Reconstruction
 Free-Style Free Perforator Flaps in Lower Extremity Reconstruction
Free-Style Free Perforator Flaps in Lower Extremity Reconstruction
 Free Flaps in Lower Extremity Reconstruction
Free Flaps in Lower Extremity Reconstruction
 Orthoplastic Approach to Lower Extremity Reconstruction
Orthoplastic Approach to Lower Extremity Reconstruction
 The Anterolateral Thigh Perforator Flap
The Anterolateral Thigh Perforator Flap
 Lower Extremity Reconstruction in the Pediatric Population
Lower Extremity Reconstruction in the Pediatric Population
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


