Fig. 28.1
(a) Clinical picture of a high-energy penetrating injury. Notice the avulsive injury producing a composite defect characterized by loss of both soft and hard tissues. (b) CT demonstrating the hard tissue damage caused by high-velocity penetrating injury. (c) Clinical picture of the same patient after treatment which includes restoring facial form. (d) CT scan demonstrating reduction and fixation of facial fractures with restoration of facial form
Low-energy penetrating injuries, such as a knife, machete, or other sharp objects, result in isolated damage to the soft tissue or a combination of damage to the soft tissue and facial fractures, generally with preservation of soft and hard tissue masses (Fig. 28.2a, b).

Fig. 28.2
(a) Low-energy penetrating injury results in isolated damage to the soft tissue. (b) Notice the preservation of soft tissue mass after repair
28.2 Structures at Risk for Injury
Maxillofacial injuries, while not generally life threatening, present challenging problems to trauma surgeons because of the concentration of complex, vital anatomic structures with their associated functions. These structures include the brain with its 12 cranial nerves, 4 of the 5 senses, the airway, an intricate bone configuration, the cervical spine, the major blood vessels, the salivary glands, and the centers for speech and deglutition. In addition, the face has an important esthetic component that affects patients’ self-worth and psychological well-being.
28.3 Goals of Management
Penetrating maxillofacial injuries do not usually create major resuscitation challenges. As such, immediate attention needs to be directed toward evaluating and managing the airway and bleeding. After the patient is stabilized, the long-term treatment objectives are to restore facial form and function (Fig. 28.1c, d) while preventing or minimizing complications, e.g., infection, inadvertent damage to the facial nerve, or discarding valuable soft or hard tissue structures.
The purpose of this chapter is to highlight the principles of evaluation and management of patients with penetrating maxillofacial injuries focusing on the acute management skills required by the trauma surgeon and the latter management issues addressed by the specialty service.
28.4 Acute Management
28.4.1 Patient Evaluation
Most maxillofacial injuries are not life-threatening and are usually evaluated as a component of the secondary trauma survey. Airway and bleeding, however, require immediate evaluation and control. Simultaneously, the clinician must avoid unnecessary manipulation of the neck pending cervical spine clearance. Ten percent of facial penetrating injuries associated with a motor vehicle collision (MVC) or fall from height have associated cervical spine injuries.
Other potential complications initiated during the initial evaluation and management are due to inappropriate management of the maxillofacial soft and hard tissues. For example, careless vessel clamping and ligation while trying to obtain homeostasis may result in facial nerve damage. Direct pressure often provides adequate homeostasis. Discarding nearly avulsed tissues, especially those involving the eyelid, may result in soft tissue defects that are challenging to correct. Discarding fracture segments could impair subsequent early or late treatment (Fig. 28.3).

Fig. 28.3
Frontal repose view of frontal bone deformity as a result of discarded hard tissue at the time of neurosurgical treatment
28.5 Airway Management
Airway control is a priority. Obstruction may be due to foreign bodies, e.g., dentures, teeth, fluids (blood or vomit), soft tissue (tongue or loss of tongue support due to a mandible fracture), or direct laryngeal injury. While assessing the airway, bleeding from maxillofacial injuries can be managed acutely with pressure and local hemostatic measures.
Primary airway management is a core competency of the trauma surgeon and addressed in detail elsewhere in text. There are a few considerations worth noting when managing the airway of patients with maxillofacial injuries. Usually, the initial airway control is by endotracheal intubation or performance of a surgical airway. With few exceptions, at a later stage and depending on oral endotracheal tube that needs to be converted to the maxillofacial operative procedure, the orotracheal intubation is changed to nasotracheal or converted to tracheostomy. Occasionally, maxillofacial surgeons can work around an oral airway or may elect to perform submental intubation (Fig. 28.4a, b).

Fig. 28.4
(a) Extraoral and (b) intraoral views of submental intubation. Arrow points to endotracheal tube as it enters the floor of the mouth
28.6 Evaluation and Management of Maxillofacial Bleeding
Penetrating injuries of the face may bleed profusely due to the highly vascular nature of this region. The corollary of this is that injuries to hard or soft tissues are more likely to survive and be resistant to infection. Many times, because of the copious blood supply and relatively small wounds, maxillofacial injuries appear serious. As such, it is critical to clean the wounds, to establish the nature and severity of the injuries, and to identify and control bleeding sources. Magnification (loupes) and illumination (headlights) are invaluable to assist in identifying and controlling bleeding. Direct pressure is effective for controlling bleeding from facial injuries. The wounds can be cleaned efficiently with sponges soaked in saline or dilute hydrogen peroxide.
Nasal injuries associated with bleeding are common and can be challenging to manage. Injury of Kiesselbach’s plexus accounts for nasal bleeding in 90 % of the cases. Nasal bleeding can be caused by laceration of the nasal mucosa, and any of the nasal vessels can be the source of the bleeding. Since the branches of the internal maxillary artery and the anterior and posterior ethmoidal arteries are located in the posterior aspect of the nose, most likely that these vessels will cause posterior bleeding toward the pharynx and anterior packing of the nose or packing of the oral cavity is ineffective. As such, posterior nasal packing is indicated. Posterior packing consists of placing a Foley catheter into the far posterior portion of the nasal cavity and then inserting an anterior nasal pack in front of the balloon. The posterior pack is maintained for 1–3 days (Fig. 28.5a).

Fig. 28.5
(a) Typical blunt midface injury demonstrating stabilization of the neck with a cervical collar, oral intubation, facial edema, periorbital ecchymoses, and posterior nasal pack (Foley catheter) and anterior nasal pack to control nasal bleeding. Marked facial edema develops within a few hours of injury, making the physical examination more difficult. (b) Same patient few days later. Notice the decreased swelling allows better delineation of the deformity and facilitates operative repair of the injuries
Nasal septal hematomas are associated with septal fractures. Septal hematomas need to be diagnosed and managed efficiently. Left untreated, a septal hematoma may produce necrosis of the underlying cartilage, producing a nasal deformity characterized by collapse of the nasal dorsum and may be very difficult to correct.
Management of the maxillofacial bleeding can be achieved by any one or a combination of the following options:
- 1.
Direct pressure:
Bleeding from maxillofacial injuries responds well to direct pressure. Use dry sponges and abdominal swabs, and press on the bleeding site to produce pressure hemostasis (Fig. 28.6).

Fig. 28.6
Hemostasis obtained by packing the wound with sponges
- 2.
Ligation:
Ligating vessels is done in the usual manner; however, avoid blind clamping of tissues to prevent iatrogenic injury to vital structures such as the facial nerve.
- 3.
Hemostatic agents:
Incremental measures to obtain homeostasis include packing with hemostatic agents, e.g., oxidized cellulose, microfibrillar collagen, and chitosan-based hemostatic dressing.
- 4.
Interventional radiology:
Occasionally, bleeding from the nose and infratemporal fossa or indeterminate, profuse maxillofacial bleeding cannot be controlled with usual methods. Under these circumstances, consider consultation with interventional radiology for diagnostic angiography and embolization.
28.7 History and Physical Examination of Maxillofacial Injuries
In most cases, evaluating maxillofacial injuries is a component of the secondary trauma survey. Historical information regarding the mechanism of injury, timing, and location of injury can be valuable. Unless the patient is awake and oriented, these data are best collected from witnesses of the incident. Medical history may be important, and family members are helpful with an unconscious or intubated patient. The simplest way to ascertain quickly if there is a fracture of the maxilla or mandible is to ask patients if their bite is altered. If the answer is yes, there is a high likelihood of a fracture. If the answer is no, there is a low likelihood of fracture. The following paragraphs outline a method for completing the initial examination for maxillofacial injuries.
28.8 External Examination
The goal of the examination is to determine quickly and efficiently the presence or absence of maxillofacial injuries. Edema develops within a few hours after injury, masking underlying injuries, making physical identification of injuries more difficult (Fig. 28.5a).
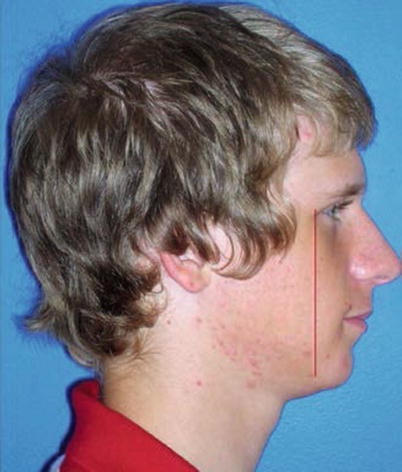
Inspect the scalp and face for obvious lacerations or deformities. Probe the laceration to determine if it communicates with the underling bony structures. Assess facial nerve function by asking patients to raise their eyebrows, squeeze their eyes shut, smile, pucker their lips, and grimace. Lacerations posterior to a line dropped perpendicular to the horizontal at the lateral canthus of the eye increase the risk for a facial nerve or salivary duct injury (Fig. 28.7).