Introduction
This chapter covers a selection of pedicled flaps commonly used for soft tissue coverage of the hand. Several are based on primary vessel pedicles (Moberg flap, posterior interosseous artery flap, and homodigital island flaps), whereas others are based on secondary cutaneous branches of larger primary structures (ulnar artery perforator flap, cross finger flap). These provide a less complex and rapid means of achieving wound closure as compared with free tissue transfer, and often with very low donor site morbidity. As a result, these have become “workhorse” flaps for the reconstructive hand surgeon.
First Dorsal Metacarpal Artery Flap
Flap Anatomy ( Fig. 45.1 and See Fig 12.20 , Fig 12.21 , Fig 12.22 )
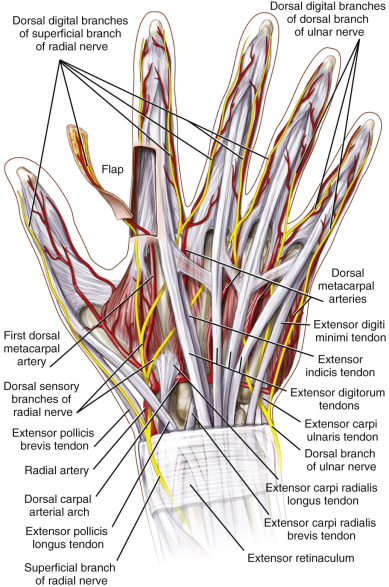
The dorsal carpal arch originates from the dorsal branch of the radial artery as it courses through the anatomic snuffbox. The arch gives rise to a series of dorsal metacarpal arteries that travel distally in the intermetacarpal spaces. These vessels are numbered sequentially from radial to ulnar (first, second, third, etc.). The vessel that has been referred to as the first dorsal metacarpal artery (FDMA) will often arise independently from the radial artery rather than as a branch of the dorsal arch itself. This vessel runs along the surface of the first dorsal interosseous muscle to ultimately provide perfusion to the skin overlying the dorsal aspect of the index finger proximal phalanx.
Dominant Pedicle:
first dorsal metacarpal artery
Length: 3–6 cm
Diameter: 0.5–1.0 mm
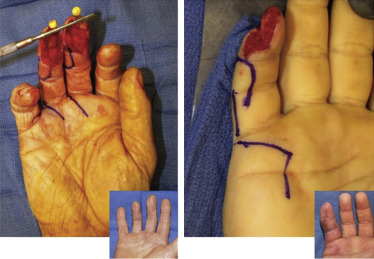
The vascular pedicle is often clearly visible proximal near the pedicle origin in the snuffbox, whereas its terminal branches are often difficult to discern. These branches pass between the extensor tendon and the radial mid-axis of the index finger. Wide harvest of this entire fibrofatty leash to include all tissue immediately subdermal down to, but not including, the sagittal fibers of the extensor mechanism is performed to safely include these small vessels. From the metacarpophalangeal (MCP) joint to the proximal interphalangeal (PIP) joint, the skin paddle is harvested with all of the subcutaneous fat and vessels, leaving only the thin paratenon covering the extensor mechanism.
Minor Pedicle:
communicating perforators from palmar arterial system
The first dorsal metacarpal artery communicates with the palmar arterial systems through a communicating branch reliably located at the level of the metaphyseal flare of the index finger metacarpal neck. This vessel is routinely ligated in the elevation of the antegrade FDMA flap, but may be used as a pivot point for a retrograde distally based FDMA flap (utilized if coverage is needed for the proximal phalanx or PIP joint).
Venous Drainage (See Fig 12.18 , Fig 12.22 )
Primary:
venous comitantes of the FDMA system
Length: 3–6 cm
Diameter: 0.2–0.3 mm
These vessels are particularly difficult to identify. The pedicle is harvested with a wide fibrofatty leash that encompasses the subcutaneous fat, vessels, and fascia overlying the first dorsal interosseous muscle. This wide margin of harvest will ensure adequate drainage to the skin segment.
Secondary:
branch(es) of the cephalic venous system
Length: range 3–6 cm
Diameter: range 1–2 mm
Larger caliber superficial branches of the cephalic system can be harvested to be included in the vascular leash if they course appropriately to the skin segment and can be mobilized adequately. This may provide additional drainage if desired.
Flap Innervation ( Fig. 45.1 and See Fig 12.20 , Fig 12.22 )
Sensory nerve branches from the dorsal sensory radial nerve will typically be included in this flap, particularly if volar thumb coverage is desired. There is a reliably located branch that will mimic the course of the FDMA, although it is located more superficially. This can be elevated and mobilized with the flap to provide immediate sensation of the reconstruction.
Flap Components: Skin and Subcutaneous Tissue
Advantages
- •
Reliable anatomy
- •
Ease and speed of harvest
- •
Sensate thin pliable tissue
- •
Low donor site functional morbidity
Disadvantages
- •
Donor site requires skin graft
- •
Donor site visibly conspicuous
Flap Design ( Cases 45.1 , 45.2 )
The skin segment of the flap may encompass the entire dorsal skin of the proximal phalanx of the index finger. Although typically described as a rectangular flap, the authors routinely make two modifications on this design. First, the proximal ulnar margin of the flap may be rounded to avoid incisions violating the second web space in order to avoid scar contractures in this region of unique tissue. Second, the proximal radial margin can be harvested with a tapering V-shaped tongue of skin. This tapered edge will allow ease of inset of the flap in its destination by relieving the tension of the skin margin on the distal tunnel.
As with most fasciocutaneous flap harvest techniques, the flap is generally harvested slightly larger than the measured soft tissue defect to ensure tension-free closure. Regardless of size of the harvest, the donor site will require skin graft coverage and cannot be primarily closed.
Particular care should be made to design the radial margin at the glabrous margin of the index finger radial midaxis. Designing this margin more dorsally may risk compromising the pedicle connections to the skin segment.
After outlining the skin segment as described, a longitudinal incision is then extended from the proximal margin of the skin flap to the palpable interval between the thumb and index metacarpal bases.
Prior to tourniquet inflation, the surgeon may elect to discern the pathway of the FDMA with a handheld Doppler. This is not required and the authors do not routinely perform this evaluation. Even in the absence of an audible Doppler signal in this region, the flap may be successfully harvested.
Flap Dimensions
Length: 3 cm (range 2–5 cm)
Width: 2 cm (range 1.5–3 cm)
Thickness: the thickness of the dorsum of the hand
Anesthetic Considerations:
local anesthesia with tourniquet and some sedation can be used.
Technique of Harvest
After exsanguination and tourniquet inflation, the preoperative markings described above are incised. The flap may be elevated from distally to proximally. The skin segment is elevated immediately above the paratenon of the extensor tendon on all margins except the proximal margin that contains the pedicle. On the radial margin the subcutaneous tissue is harvested to include all tissue immediately dorsal to the radial digital artery and nerve of the index finger. As the MCP joint is approached, the dissection cautiously proceeds immediately superficial to the sagittal bands, taking great care not to disrupt the vascular leash.
The skin flaps at the metacarpal level are elevated in the subdermal plane in both a radial and ulnar direction. Once adequate exposure is obtained, the subcutaneous tissue is incised sharply along the radial margin of the index metacarpal to the subfascial plane of the first dorsal interosseous muscle. On the radial margin of the dissection the subcutaneous tissue is incised sharply down to the subfascial plane of the adductor pollicis muscle. All intervening tissue between these parallel boundaries is then elevated distal to proximal, exposing the two muscles subfascially.
At the level of the index metacarpal neck the communicating branch to the volar arterial systems is identified and ligated, permitting further elevation of the leash proximally. The FDMA can now be visibly identified on the undersurface of the muscle fascia as the elevation continues to the level of the snuffbox. The origin of the vessel can usually be clearly identified emanating from the radial artery.
On the superficial surface of the leash the superficial veins and sensory nerve branch from the radial sensory nerve can be identified. These structures can be dissected to further enable further mobilization of the pedicle. At no point is the arterial pedicle skeletonized in order to avoid venous compromise of the flap.
At this point, it is wise to release the tourniquet and confirm viability of the flap as assessed by subdermal bleeding at the distal flap margins. This can provide the surgeon with reassurance to proceed with wound preparation and creation of a tunnel for passage of the flap.
With the tourniquet reinflated, the wound is now widely debrided and a subcutaneous tunnel is created to generously accommodate the neurovascular leash. When covering a dorsal or volar thumb defect (most common indications for this flap), the wound may be extended with a 1–2 cm incision along the apex of the tunnel to diminish the pressure on the pedicle near the flap inset. In this extension of the wound, the proximal V-shaped flap margin (see above) may provide tension-free coverage and inset closure. Alternatively, the entire tunnel may be opened to allow ease of inset and closure.
Donor Site Closure
The donor site incision over the dorsal metacarpal region may be easily closed primarily. The defect over the proximal phalanx is then skin grafted from the surgeon’s preferred donor site. The authors will typically harvest from the thin pliable skin of the visibly inconspicuous medial brachium.
Indications:
distal dorsal and volar thumb defects
Small wounds over the MCP joints or first web space where it has adequate pedicle length to reach the MCP joints of the middle finger and thumb.
Postoperative Care and Outcomes
The donor site may be covered with a bolster dressing or bulky secure soft dressing and a splint for 7–10 days to ensure skin graft survival. Thereafter, splinting may be abandoned and motion-enhancing exercises commenced. The skin graft usually survives without difficulty in this location, and stiffness of the donor index finger is very rare in this procedure.
The skin-grafted donor site will display a contour defect initially due to the thin nature of the skin graft. With time and scar maturation the contour remarkably normalizes, but the color differences between the skin graft and the dorsal finger remain noticeable. The donor site typically becomes pain free and full motion is usually regained (see Cases 45.1 , 45.2 ).
Cross Finger Flap
Flap Anatomy ( Fig. 45.1 and See Fig 12.20 , Fig 12.21 , Fig 12.22 )
Cross finger flaps are designed for coverage of soft tissue defects on the volar aspect of the digits. The cross finger flap is an interpolated flap; it is raised as a pedicled skin flap on the dorsal aspect of a finger adjacent to the digit requiring coverage, inset by temporary attachment of the two fingers, and divided weeks later when perfusion to the transferred skin is capable of being supported by the recipient finger. Unlike the other flaps described in this section, the cross finger flap always requires a second-stage procedure for division of the pedicle.
The donor site is the dorsal aspect of the digit distal to the PIP joint. This angiosome is perfused by dorsal branches of the digital artery. These very small vessels pass from the volar aspect of the finger through Cleland’s ligament into the dorsal skin. The flap is not designed to be harvested as an island flap nor is the pedicle skeletonized. As a pedicled flap the size of the elevated skin segment dictates the reach of the flap; pedicle length and caliber are neither defined nor relevant to harvest.
Dominant Pedicle:
dorsal skin branches of the donor digital artery
These branches course dorsally at the level of the proximal portion of the middle phalanx within the subcutaneous tissue.
The flap is designed to incorporate a wide base of the entire length of the middle phalanx in an effort to avoid injury to these vessels.
Venous Drainage (See Fig 12.16 , Fig 12.22 )
Venous drainage of the flap is provided by the small venous comitantes of these dorsal arterial branches and is incorporated within the flap harvest.
Flap Innervation
This flap is most frequently transferred as an insensate flap. However, dorsal sensory branches of the ipsilateral digital nerve may be dissected proximally on the donor finger, transected, and coapted to the digital nerve on the recipient finger in an effort to provide sensate reconstruction.
Flap Components
This flap is most commonly harvested as a skin flap for volar adjacent digital coverage. A modification, the “reversed cross finger flap,” may be harvested as a layer of subcutaneous fibrofatty tissue only. This would be designed to provide coverage of dorsal wounds on adjacent fingers.
In the conventional cross finger flap, the donor site requires skin graft coverage. In the “reversed cross finger flap,” the donor site skin layer is closed primarily and the recipient site requires skin graft coverage over the flap.
Advantages
- •
Ease of harvest
- •
Reliable anatomy and durability
- •
Thin pliable tissue
- •
Possibility for sensation if nerve coaptation performed
Disadvantages
- •
Requires two operative stages
- •
Immobilization period risks stiffness of both recipient and donor digits
- •
Conventional flap is insensate if nerve coaptation is not feasible
- •
Donor site skin graft is visibly conspicuous
Preoperative Preparation
If the donor finger is uninjured, no preoperative testing is necessary. If the donor finger is also injured, a surface Doppler examination is recommended to ensure that the digital artery on the adjacent side of the donor finger is patent and uninjured.
Flap Design ( Cases 45.3 , 45.4 )
Flap design is dictated by the location of the wound and the ease of reach of the tissue on the adjacent digits. The most common applications are for coverage of fingertip wounds, or wounds over the DIP joint flexion crease. Due to the distal location of these wounds the longer of the adjacent digits is usually selected to provide the greatest reach of the flap without tension. For this reason, the middle finger often serves as the donor for wounds on either the index or ring fingers. Alternatively, wounds on the middle and small fingers are usually covered by flaps harvested from the ring finger.
The index finger may serve as a donor for thumb wounds, although this is not commonly performed because the variety of other better options for volar thumb coverage (FDMA flap and Moberg flap), and the morbidity of immobilizing a traumatized hand with the thumb maximally adducted (first web space contracture).
Although commonly described as a rectangular flap harvested by outlining the skin on the dorsal aspect of the proximal phalanx, the authors routinely design this flap in a trapezoidal fashion. This is achieved by creating two parallel incisions for the proximal and distal margins of the flap. These are created to migrate distally as they cross the dorsal aspect of the donor finger and are ultimately joined by a midaxial incision on the contralateral aspect of the donor digit. This design harvests tissue more distally than the conventional rectangular design, including some skin over the DIP joint extension crease. The eponychial fold is not disturbed. This design modification may be used particularly effectively when distal reach of the flap is required, such as for fingertip coverage or on DIP joint flexion crease wounds on the middle finger.
Flap Dimensions
Length: 3–4 cm
Width: 1.5–2.5 cm
Thickness: 1.5–3 mm
Flap Markings
After selecting the adjacent donor digit, the markings start at a point on the adjacent midaxis of the digit at the level of the PIP joint. An oblique line is then created moving distally as it approaches the contralateral midaxis. Here a longitudinal line is drawn to the level of the base of the distal phalanx (proximal to the eponychial fold, but distal to the DIP joint extension crease). The third side of the flap is then drawn retreating to the ipsilateral midaxis of the donor digit, running parallel to the oblique proximal flap margin. The starting point of this drawing is made just dorsal to the midaxis in an effort to avoid compromising the passage of the dorsal vascular branches of the digital artery that supply the flap. The endpoint of the flap drawing is positioned volar to the midaxis in an effort to make the flap base less kinked upon inset to the adducted recipient finger.
Anesthetic Considerations
This flap can be performed under local anesthesia with sedation routinely. However, it may also be easily performed without sedation using a local digital block for the donor and recipient fingers and a field block for the skin graft preferred harvest site. The authors will typically harvest from the thin pliable skin of the visibly inconspicuous medial brachium.
Technique of Harvest
The authors will typically harvest this flap using a forearm tourniquet under local anesthesia. According to surgeon’s preference, however, the flap may be harvested without tourniquet, or with tourniquet applied at a different location. The forearm level tourniquet is easily tolerated by the awake patient for the brief duration of the procedure. Lidocaine with epinephrine may be used for skin graft harvest above the tourniquet at the medial brachium. If the surgeon prefers donor sites distal to the tourniquet, epinephrine may not be required.
After inflation of the tourniquet and successful local blocks, the wound is debrided to healthy margins. The attention is then turned to the donor digit. The flap is designed as described above. Incisions on all three sides are made to the depth immediately above the filmy paratenon of the extensor mechanism. The flap is mobilized and unfurled to provide coverage of the adjacent volar digital wound.
The authors will typically harvest and inset the skin graft on the paratenon of the donor wound first using dissolvable suture. The flap is then inset and sutured to the adjacent digit with as minimal tension as possible. Attempts are made to inset thoroughly on three sides so that there is as much linear contact area for vessel ingrowth as possible prior to subsequent division.
Tension-free inset may require flexion of the recipient digit PIP joint if the wound is very distal. This should be minimized as much as possible.
Flap Handling
The flap and skin graft sites are covered with a protective splint to protect the attached digits during and prior to the next surgery. The period between flap inset and division is tailored to the patient and situation. While it may typically be divided as early as 2 weeks after inset, longer periods (i.e., 3 weeks) may be desirable if the patient is a smoker or has subnormal perfusion of the recipient digit. Alternatively, shorter periods are more desirable in patients with higher risk of digital stiffness (osteoarthritic or elderly patients).
Flap division is performed under local anesthesia. No preoperative testing is required. The base of the flap may be sharply divided and then inset on both the donor and recipient fingers quite rapidly. The digits may then be mobilized immediately unless other traumatic requirements limit motion (i.e., fractures and tendon repairs).
Flap Modification
The reversed cross finger flap modification as described above is harvested similarly with the goal of covering dorsal wounds on adjacent digits. The design for this flap is conventionally rectangular, rather than trapezoidal. The skin is elevated on three sides in the subdermal plane to be mobilized away from the injured digit. The fibrofatty tissue is then elevated on three sides in the opposite direction to unfold onto the injured digit. Once inset, the donor skin is then returned to its native position to cover the donor site, and the skin graft is applied to the recipient digit on top of the flap tissue.
Outcomes
The cross finger flap has been a conventional workhorse flap because of its reliability and ease of harvest. The skin will shape and mature to the contour of the digit effectively. The donor site skin graft reliably survives without difficulty if the paratenon is carefully preserved during harvest.
One of the drawbacks of the flap is the lack of sensation, particularly for fingertip reconstruction. The dorsal digital nerve may be coapted to the recipient digital nerve; however, this may not be feasible depending on the condition of the recipient digit tissue. This technique also requires the time and inconsistency of digital nerve regeneration. The second major drawback is the risk of stiffness in both the injured and donor fingers during required immobilization, particularly in the elderly or arthritic population. For these two reasons, the authors have preferred the advantages of the homodigital island flap for fingertip reconstruction when feasible (see Cases 45.3 , 45.4 ).
Moberg Flap
Flap Anatomy (See Figs 12.17 and 21.22)
The thumb neurovascular volar advancement flap, or Moberg flap, is designed to provide immediately sensate, single-stage glabrous skin coverage for soft tissue defects of the volar pulp of the thumb. The flap is harvested with both the radial and ulnar digital neurovascular bundles and advanced distally to reconstruct digital tip injuries. The flap may be reliably performed only on the thumb due to the thumb’s robust dorsal blood supply that enables the skin to survive despite harvest of both volar neurovascular bundles with the flap.
Dominant Arterial Pedicle:
radial and ulnar digital arteries of the thumb
Length: 1–2 cm advancement with island design
Diameter: 1–1.5 mm
Venous Drainage (See Fig. 12.10 ):
venous comitantes of the radial and ulnar digital arteries
Innervation (See Fig. 12.10 ):
immediate sensation to the flap is provided by the radial and ulnar digital nerves that are carefully included in the flap elevation
Advantages
- •
Glabrous soft tissue of appropriate thickness and quality for tip reconstruction
- •
Single stage procedure
- •
Immediately sensate coverage
- •
Reliable and durable flap
- •
Ease and speed of harvest
Disadvantages
- •
Limited ability to cover larger defects of volar pad (>2 cm).
Preoperative Preparation
No preoperative testing is required. If the thumb has sustained a second, more proximal laceration, the condition of the digital vessels should be assessed with a surface Doppler to ensure safety of harvest.
Flap Design ( Cases 45.5 , 45.6 )
The flap is designed by making two parallel markings on the midaxes of the thumb extending from the wound to the MCP flexion crease. These markings should reliably be dorsal to the pathway of the neurovascular bundles.
This flap has been described as a pedicled flap performed without additional incisions. It has been described as a V-Y advancement flap that requires a tapered proximal “V-shaped” incision connecting the midaxial incisions. It has been described as an island flap that requires a transverse incision at the MCP flexion crease with the goal of advancing the flap and skin grafting the donor defect at the flexion crease. The technique is selected by surgeon’s preference. The authors routinely perform the last of these choices because they find it enables the greatest advancement and tension-free closure of the donor site.
Flap Dimensions
The skin island includes the entire glabrous volar surface of the thumb. It may be 2–3 cm wide and its length varies with the side of the length of the digit and the size of the tissue lost. The proximal border of the flap is the MCP flexion crease.
Anesthesia Considerations
This flap can be performed under local anesthesia with sedation routinely. However, it may also be easily performed without sedation using a local thumb digital block and a field block for the skin graft preferred harvest site. The authors will typically harvest from the thin pliable skin of the visibly inconspicuous medial brachium.
Technique of Harvest
The authors will typically harvest this flap using a proximal bicep tourniquet under local anesthesia with sedation. According to surgeon’s preference, however, the flap may be harvested without tourniquet, or with forearm level tourniquet with only local anesthetic utilized. The forearm level tourniquet is easily tolerated by the awake patient for the brief duration of the procedure. Lidocaine with epinephrine may be used for skin graft harvest above the tourniquet at the medial brachium in this circumstance.
After inflation of the tourniquet, the wound is debrided to healthy margins. Attention is then turned to the flap elevation. Two midaxial incisions are created and dissection continues dorsal to the neurovascular bundles and volar to the flexor tendon sheath. This continues to the level of the MCP flexion crease.
At this point, the flap can be manually advanced to determine if further dissection is necessary. Flexion of the IP joint of the thumb in order to achieve distal reach of the flap has been shown to be well tolerated without subsequent development of flexion contractures.
The advancement is often inadequate without performing a proximal incision and mobilization. If this is required, it may be performed in a tapered “V-shape” to permit V-Y closure of the donor site with flap advancement. Alternatively, the proximal incision can be performed transversely at the MCP flexion crease and a skin graft can be used for coverage of the defect created by flap advancement.
Skeletonization of the digital bundles should not be performed. This is avoided to protect the venous comitantes and minimize the risk of flap congestion. However, mobilization of this neurovascular leash should be performed in two planes to maximize advancement. The first is in the immediately subdermal plane proximal to the flap on the volar thenar eminence. This liberates the subcutaneous tissue from the less pliable thenar skin. The second plane is immediately above the flexor sheath and muscle fascia proximal to the flap. This is done with extreme care to avoid injury to the neurovascular structures. These two dissection planes will maximally mobilize the intervening layer and gain maximal tissue advancement.
Flap Handling
Once elevated, the flap is inset on the radial and ulnar margins first, using each suture to advance the flap distally. The pulp is then able to be inset in a tension-free manner with maximal advancement achieved. Sutures should not be placed into the distal nailbed so that tension does not result in a hook-nail deformity. If enough advancement is achieved the two distal corners of the flap may be sutured approximated together to create a convex prominence of the distal tissue to re-create the volar pad of the thumb.
Donor Site Closure
The skin graft is inset into the donor defect with dissolvable suture. A bulky dressing and thumb spica splint are used to immobilize the reconstruction for 7–10 days. Motion may thereafter commence unless concomitant injuries prohibit movement (i.e., fractures, tendon repairs).
Outcomes
This flap is a workhorse flap for volar thumb defects because it is a hardy and reliable flap that routinely provides immediately sensate tissue on the critically important thumb pad. The reconstruction tends to contour and mature into an excellent functional and aesthetic outcome routinely. Flexion contractures of the IP joint are rare, even if IP joint flexion is used to enable flap advancement. Skin graft adherence and survival is routine, and the lack of sensation at the skin graft site is well tolerated in the MCP joint flexion crease.
A common risk is hook-nail deformity and can be avoided if sutures are not placed in the nailbed during flap insetting. Additionally, if any portion of the distal phalangeal bone has been lost, the nailbed should be trimmed to the level of the bone. Preservation of nailbed without osseous support will increase the risk of hook-nail deformity (see Cases 45.5 , 45.6 ).
The Homodigital Island Flap
Flap Anatomy (See Fig 12.17 , Fig 12.20 , Fig 12.21 , Fig 12.22 )
This adipocutaneous neurovascular island flap can be raised from the distal volar radial or volar ulnar aspect of the digit. The flap is designed so that a portion of it lies directly over either the radial or ulnar neurovascular bundle. The arterial supply to the flap is the proper digital artery. As there is rarely a sizeable vein running with the artery, the venous drainage of the flap is likely a fine network of perivascular veins. The flap contains within it either the proper radial or ulnar digital nerve. As such, it provides immediate sensibility to the reconstructed digit.
Dominant Pedicle:
proper radial digital artery or proper ulnar digital artery
Length: 3–6 cm
Diameter: 1.0–1.5 mm
Identification of the digital neurovascular bundle can be achieved through either a Bruner or midlateral incision. The proper digital artery and nerve will be encountered by releasing Grayson’s and Cleland’s ligaments. Care should be taken to minimize disruption of the fine perivascular venous network by not skeletonizing the neurovascular bundle and by avoiding separation of the artery from the nerve. Small dorsal arterial and nerve branches identified at the level of the middle phalanx and distal aspect of the proximal phalanx should be liberated with a microbipolar cautery as they could tether the flap and ultimately limit advancement. If possible the large dorsal arterial and nerve branches that often arise at the proximal aspect of proximal phalanx should be preserved.
Minor Pedicle:
transverse digital palmar arch.
Three separate transverse digital palmar arches provide vascular communications between the radial and ulnar digital arteries. These arches are named the proximal, middle, and distal transverse digital palmar arch, corresponding to their location in the finger. The small vascular interconnections of the middle and distal arches can support a retrograde homodigital island flap that can be raised without the corresponding digital nerve (the benefits of harvesting a digital nerve or dorsal nerve branch with the retrograde flap are debated). The location of middle arch at the distal cruciate pulley provides a favorable pivot point that allows a flap raised from the volar proximal phalanx to often reach the distal phalanx without the need to flex the interphalangeal joints. The vessels of the arch are quite small and could be easily injured if direct visualization or skeletonization were attempted. To avoid injury to the middle arch vessel when raising the retrograde homodigital island flap, dissection should stop 5 mm proximal to the distal interphalangeal joint.
Venous Drainage (See Fig. 12.22 )
Primary:
fine perivascular venous network
Length: 3–6 cm
Diameter: Submillimeter (not often visible)
These vessels are rarely visible. Care should be taken to minimize disruption of the fine perivascular venous network by not skeletonizing the neurovascular bundle and by avoiding separation of the artery from the nerve.
Secondary:
none
Length: none
Diameter: none
Flap Innervation (See Fig 12.21 , Fig 12.22 )
The anterograde flap contains within it a proper digital nerve and is immediately sensate.
Advantages
- •
Single-stage operation
- •
Reliable anatomy
- •
Ease of harvest
- •
Delivery of sensate glabrous tissue
- •
Low donor site morbidity
- •
Well-hidden scars if harvested from the ulnar aspect of the digit
Disadvantages
- •
Donor site requires skin graft
- •
Possibility of proximal interphalangeal joint contracture
Flap Dimensions
Skin Island Dimensions
As the maximum size of this flap has not yet been studied, these measurements reflect the authors’ experience.
Length: Average 1.5 cm (range 1.0–2.0 cm), primary closure not recommended
Width: Average 1.0 cm (range 0.5–1.5 cm), primary closure not recommended
Thickness: Average 1 cm (range 0.5–1.5 cm)
Flap Markings
A template of the defect is made and the dimensions of the flap measured ( Fig. 45.8 ). The template is transposed over intact skin just proximal to defect. The template should be positioned over the course of either the radial or ulnar digital neurovascular bundles. The long axis of the template should be oriented in the same direction of the long axis of the defect to minimize rotation or twisting upon inset after advancement.