Pedicled and Free Groin Flap
Mark Morris
Kevin C. Chung
DEFINITION
A free flap requires the transfer of tissue from one body site to another, with anastomosis of arterial and venous systems to the recipient site using microsurgical techniques.
A pedicled flap transposes tissue from a donor site to a recipient site while keeping the tissue partially attached to the donor site. The donor vascular pedicle is left intact to supply the flap. Pedicled flaps are reliable and do not require microsurgery.
The groin flap was described in 1972 by McGregor and Jackson1 for reconstruction of soft tissue defects of the hand. This was once a “workhorse” flap for hand reconstruction; however, with the introduction and advancement of microsurgery, it has fallen out of favor for many indications. Nevertheless, there are still many indications for its use.
When a pedicled groin flap is used, patients must be counseled that they will require multiple operations (average 4.6 operations per patient), including flap division, debulking, and tissue rearrangement for contouring.2
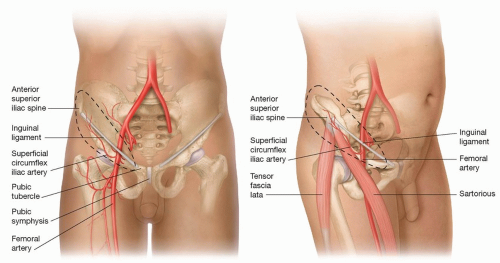 FIG 1 • Vascular and regional anatomy of the groin flap, which follows the axis of the superficial circumflex iliac artery. |
ANATOMY
The groin flap is based on the superficial circumflex iliac artery (SCIA).
The SCIA arises approximately 2 to 3 cm distal to the inguinal ligament, either directly from the femoral artery (70%) or from the superficial inferior epigastric artery (FIG 1).
The SCIA passes laterally from its origin and gives a deep branch at the medial border of the sartorius.
The superficial branch then pierces the fascia at the lateral border of the sartorius and runs 2 to 3 cm distal and parallel to the inguinal ligament, toward the anterior superior iliac spine (ASIS). This superficial branch supplies the skin to be used for the flap.
After reaching the ASIS, the superficial branch of the SCIA branches further and anastomoses with branches of the superior gluteal, deep circumflex iliac, and ascending lateral femoral circumflex arteries.
The SCIA pedicle is generally between 0.8 and 1.8 mm in diameter.3
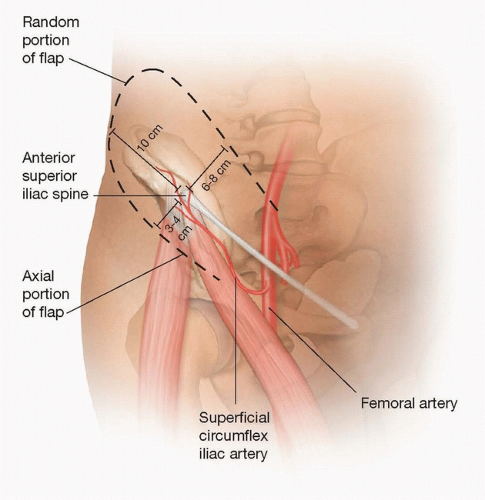
FIG 2 • Limits of the groin flap.
Venous drainage of the flap is split between the superficial circumflex iliac vein and the venae comitantes of the SCIA. Both of these eventually drain into the femoral vein, either directly or via the saphenous vein.
Flap size is limited to about 13 × 10 cm (FIG 2). The axis of the SCIA is marked by palpating the femoral pulse, marking the origin 2 to 3 cm distal to the inguinal ligament and then drawing a line to the ASIS. The flap will follow this axis.
The medial boundary of the flap is about 3 to 4 cm lateral to the femoral artery (2-3 cm medial to the medial border of the sartorius).
The maximum width of the flap that can be primarily closed in most patients is 10 cm. The flap should be positioned two-thirds superior to the vascular axis and onethird below the axis. This translates to up to 6 to 7 cm superior to the axis and 3 to 4 cm inferior to the axis.
The lateral portion of the flap should be designed with a 1:1 length-to-width ratio. This is because the portion of the flap lateral to the ASIS has a random pattern of vascularization. Therefore, because the width of the flap is limited to 10 cm, the lateral limit of the flap is then 10 cm lateral to the ASIS.
Sensation to the lateral portion of the groin flap is supplied by the lateral cutaneous branches of the 12th thoracic subcostal nerve (FIG 3).4 This nerve can be harvested with the flap to provide sensation to the hand, but a sensate nerve is infrequently used.
The 12th thoracic nerve pierces the internal and external oblique muscles and courses distally over the iliac crest, 5 cm posterior to the ASIS. Do not confuse the lateral femoral cutaneous nerve, which supplies sensation to the lateral thigh, for the 12th thoracic nerve.
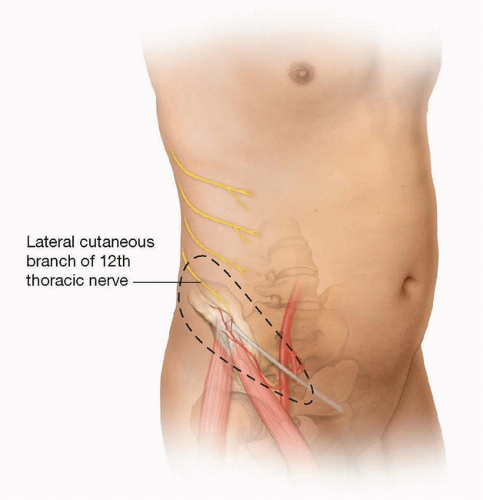 FIG 3 • The lateral cutaneous branch of the 12th thoracic nerve enters the graft opposite the vascular pedicle. |
PATIENT HISTORY AND PHYSICAL FINDINGS
History must include the mechanism of injury.
Crush and blast injuries can lead to a much larger zone of injury than expected by initial examination (FIG 4A,B).
In the case of a crush injury, the physician must also assess the patient for signs of compartment syndrome.
Contaminated wounds may require multiple irrigation and debridement procedures (FIG 4C-E).
Medical and social history—such as diabetes mellitus, peripheral vascular disease, or smoking—does not contraindicate surgery but will affect the healing potential of the flap and must be discussed with the patient.
Assess the vascular status of the remaining limb.
Motor and sensory evaluation to assess damage to nerves, tendons, or muscles.
IMAGING
Standard radiographs of the hand are done to evaluate for bony injury.
SURGICAL MANAGEMENT
Free flaps are generally considered superior to the pedicled groin flap with today’s microsurgical techniques. However, there are still many good indications for doing a pedicled groin flap:
Complex hand injuries in young children (less than 2 years). Microsurgery in infants is technically challenging because of the small size of the vessels.
In preparation for a toe-to-thumb transfer following thumb or finger loss. This preserves the recipient vessels for later microsurgery during transfer and also saves as much stump tissue as possible by providing coverage.
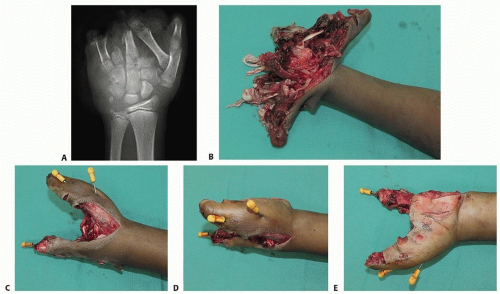
FIG 4 • A,B. Preoperative radiograph and clinical photograph, respectively, of a 12-year-old boy who sustained a bomb-blast injury to the left upper extremity. C-E. Images after left hand radical debridement, open reduction and internal fixation of the left thumb metacarpal using K-wires, and left index finger metacarpal transposition to the small finger and fixation with K-wires.Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree

 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access