Free tissue transfer is a very effective reconstructive technique for challenging defects of the head and neck and in many cases the gold standard for congenital facial paralyses and composite defects. Although its use in the pediatric population is not new and the success rates are comparable to those in adults, there is still a lack of information about its applications in children. This study aims to review the indications for use and discuss the anatomic considerations that may influence surgical complexity and long-term outcomes in the developing craniofacial skeleton.
Key points
- •
Free tissue transfer is the gold standard for reconstruction in patients with complex head and neck conditions.
- •
It is a reasonable, reliable, and largely successful option for complex reconstruction in children.
- •
Although comparable, some key differences exist between adult and pediatric free tissue transfer.
- •
Free tissue transfer in children requires appropriate consideration of the effects of reconstruction on the developing skeleton.
- •
It is important to discuss these factors and how they impact pediatric patients undergoing free tissue transfer.
Introduction
The use of free tissue transfer in the pediatric population is an area of continued interest due to its reliability for effective, single-stage reconstruction. , Its use in children was first described in the 1970s. Since then, it has gained popularity due to its high success rates. In addition to its reliability for successful reconstruction, it offers the ability to manage complex defects with consideration of function and cosmesis.
Early studies about pediatric tissue transfer surgery focused on the use of microvascular reconstruction for extremities and later expanded its use to patients with head and neck pathologies. The indications for free tissue transfer in children are comparable to those in the adult. , Although conditions that warrant free tissue transfer are similar between children and adults, these are less common in children. Consequently, there is less abundant information regarding outcomes in this patient population.
Specific risk factors impacting free flap survival in the pediatric population have been described. It has been suggested that age and flap selection may impact flap survival rates. This is most apparent in children younger than the age of 10 years due to a suspected increased risk of vasospasm due to reduced vessel caliber. , ,
Although there is a lower incidence of systemic conditions that may impact flap survival, increased difficulty due to the lower vessel caliber vessel caliber has been an area of concern. , , The use of vessels with diameters less than 0.7 mm was thought to compromise the reliability of flap uptake. , Although similar circumstances such as venous compromise can lead to flap failure, several articles suggest that arterial crisis may be more common in this population. There is also a perceived increase in technical difficulty of performing this procedure on smaller anatomic structures.
Perhaps the most important consideration in children is the impact of tissue transfer on growth of both the donor and recipient sites. , , Although the surgical technique is similar between the adult and pediatric populations, long-term functionality of the reconstruction may be affected by growth.
Additionally, the complexity of this surgery and potential impacts on the child’s physical and emotional development cannot be understated. A comprehensive discussion including a detailed description of postoperative healing, recovery times, and potential complications should be performed.
Although the utility and efficacy of free tissue transfer in pediatric patients has been previously described, some important considerations including technical difficulty in children and long-term impact on the growing craniofacial skeleton remain unclear. The goal of this article is to provide an updated review of the current literature and provide an account of the applications of free tissue transfer in pediatric patients by the senior author.
Pediatric free tissue outcomes
Free tissue transfer in pediatric patients followed shortly following its widespread adoption in adults in the 1970s. Initial concerns regarding increased risk in the pediatric population stemmed from decreased anatomic vessel diameter size, increased donor-site morbidity, challenges with postoperative management, and potential growth restrictions. Since then, several case series have validated the successful outcomes of free tissue transfer in the pediatric population. Many authors report survival rates greater than 95% routinely with fewer complications than adults. Pediatric patients have several favorable characteristics including a robust reserve to get through long anesthesia with minimal sequelae as well as better quality vessels that are typically pristine without atherosclerotic change. Systemic issues related to smoking and chronic medical conditions that typically plague the adult patients are generally not found in pediatric patients and may contribute to such high success rates despite smaller anatomy. As techniques continue to be refined, successful free tissue transfer has been reported in younger pediatric patients with the youngest performed in a patient just 10 weeks of age.
Indications
The utility of free tissue transfer for reconstruction in the pediatric population is similar to that in adults. Etiologies that require complex reconstruction include benign and malignant tumors, congenital lesions or deformities, inflammatory conditions, facial paralysis and trauma. It should be recognized that although malignancy is less common in children, the most common tumor in this population is sarcoma. This is in stark contrast with the squamous cell carcinoma that predominates in adults. The pediatric population may provide a more hospitable environment for flap survival due to a lower prevalence of malignant pathology, thus reducing the risk of preoperative radiation, and a lower incidence of systemic conditions that impact recipient vessel quality. ,
Congenital deformities that may be addressed include hemifacial syndromes and facial clefts. Many of these patients will require both soft tissue and bony components for adequate reconstruction, making a free tissue transfer such as the fibula free flap an ideal surgical choice.
Although trauma is not a common cause for micro vascular reconstruction in children, there has been documented use of free flaps for soft tissue defects secondary to burns. However, the development of more elaborate skin substitutes has limited the need for complex reconstructive surgery such as these.
Similarly, management of facial paralysis in pediatric patients constitutes a much less common indication for free tissue transfer. Chronic irreversible facial paralysis in children is overtaken in a similar manner as in adults, with initial cross-facial nerve grafting and a second-stage free-flap muscle transfer. An accelerated reinnervation of these tissues has been suggested in children as compared to adults.
Clinical considerations in pediatric population
The pediatric population presents unique challenges in obtaining successful outcomes following free tissue transfer. Extensive preoperative patient and family counseling is imperative, but despite these children typically are unable to grasp the full extent of the complexity of these surgical procedures. Adherence to head positioning instructions, activity level restrictions, as well as tolerance of enteral feeding can be difficult, unlike their adult counterparts.
Successful bony free flap reconstruction particularly of the mandible in children requires an understanding of continued growth of what is being reconstructed as well as potential morbidity that may lead to growth restriction along the donor site. Additionally, dental rehabilitation is typically mandatory in this population and thus adequate bone stock for implants must be taken into consideration.
Airway Management
Tracheostomy complications are well documented in the pediatric population. In 2 large series, tracheotomy was correlated with increased medical and total complications. Where possible, the senior author (Y.D.) prefers to avoid tracheostomy. For oromandibular cases, nasotracheal intubation is preferred. For patients under the age of 12 years and in select cases of older patients with certain intellectual disability, prolonged intubation for 3 to 4 days following surgery is employed to avoid tracheostomy and allow for postoperative swelling to subside.
Incision Design
Special attention should be paid to minimizing visible scars in the pediatric free tissue transfer patient and avoiding disfigurement with reconstructive procedures to limit any psychological sequelae as they go through schooling. In experienced hands, the ability to carry out transoral resection of neoplasms in conjunction with a minimal transcervical incision for flap inset and vessel anastomosis leads to improved esthetic outcomes in the pediatric population. A retrospective review of the senior author’s (Y.D.) cases showed a decrease in the incision size for free flap insertion from 10 cm (9–12) to 3.5 cm (2–4) over the course of 51 patients with only 5 of 33 patients requiring a lip-split incision for access.
Soft tissue reconstruction
Selection of the flap will often be determined by the size of the defect, the wound characteristics, and the functional needs of the reconstruction. For large soft tissue defects of the head and neck, the use of radial forearm free flap, anterolateral thigh (ALT) free flap, and latissimus dorsi flap has been extensively described. , Many surgeons have described a transition to the ALT free flap as the workhorse for establishment of skin coverage and oral lining as well as volume restoration. , The large size, long vascular pedicle, and ability to customize the thickness by including the vastus lateralis for adequate contouring make it increasingly attractive as a reconstructive option.
Of note, the gold standard for re-establishment of facial contour and functional smile in chronic facial paralysis in pediatric and adult populations is the gracilis free muscle transfer. Long-term outcomes including durability of smile excursion and maintenance of smile symmetry, with consideration of growth of the craniofacial skeleton, are comparable to adults.
Bony reconstruction
Growth restrictions
There is some controversy in regard to growth of the neomandible following fibula free flap reconstruction in children. Slijepcevic and colleagues found craniofacial growth complications to be as high as 23%. Guo and colleagues reported on a case series of 16 fibula free flap patients and found the fibula did not grow with the mandible. Confounding the outcomes in this study was the addition of radiation therapy and chemotherapy in 7 patients and lack of specific follow-up times determining lack of fibula growth. Hardware restriction of growth is also controversial and many authors advocate for elective hardware removal following confirmation of osseous union.
Other authors have reported growth of the fibula with the neomandible. Temiz and colleagues showed normal facial symmetry and growth in pediatric patients who have undergone fibula free flap reconstruction, suggesting growth of the neomandible along with the patient. Condyle preservation was associated with preserved growth potential of the mandible. Zhang and colleagues found a mandibular growth potential in 58.8% of patients without condyle preserved versus 81.5% with condyle preservation. Other factors of growth restriction for the neomandible include chemotherapy and radiotherapy as well as timing of surgery relative to patient age with many patients exhibiting maximal growth potential between ages of 8 and 12 years.
At the donor site, fibula flap harvest does not show impact on growth of donor leg despite fibula growth at proximal, distal and mid-epiphyseal plates. Harvest does not appear to cause ankle instability or weight-bearing issues consistent with that of the adult population. , Slijiepcevic and colleagues reported mild donor-site morbidity 1 out of 87 patients who underwent free fibula harvest.
Flap considerations
The fibula free flap is the workhorse for mandibular reconstruction in the pediatric population. Atherosclerotic disease is not seen in 3 vessel runoffs for pediatric patients, making this option almost always available. The bone stock of the fibula is adequate for dental rehabilitation. Based on existing case series, there is minimal donor-site morbidity. Fowler and Futran reported a case of valgus deformity as a late complication without obvious gait or ankle instability. Other authors described hypertrophic scar, and rare gait abnormality in one 1%.
The alternatives to the fibula free flap in the pediatric population include the vascularized iliac crest free flap and scapula free flap. These are considered second-line due to donor-site morbidity. Traction from muscle attachments at the iliac crest contribute to acetabulum development through the second decade of life and provide gait stability. For this reason, free iliac crest harvest can lead to significant gait disturbance in the pediatric population. Similarly, the scapula growth plate fuses at the end of the second decade and ossifies from superiorly to inferiorly. Harvest of the scapular tip and lateral border, therefore, can theoretically cause asymmetric growth prior to the end of adolescence. Additionally, scapula bone typically does not have adequate bone stock for implantation.
Follow-up
Given the considerations mentioned regarding potential growth restriction, pediatric free flap patients should be followed at least into early adulthood once growth is complete particularly if bony flap reconstruction is employed. Hardware complications have been reported up to 3 years out from initial surgery and follow-up with consideration of elective hardware removal is necessary if any growth restriction concerns arise. Alkureishi and colleagues published a greater than 10 year follow-up of a case series of 48 flaps, 46 of which were soft tissue, with essentially minimal long-term donor-site morbidity with high satisfaction scores. ,
Case examples
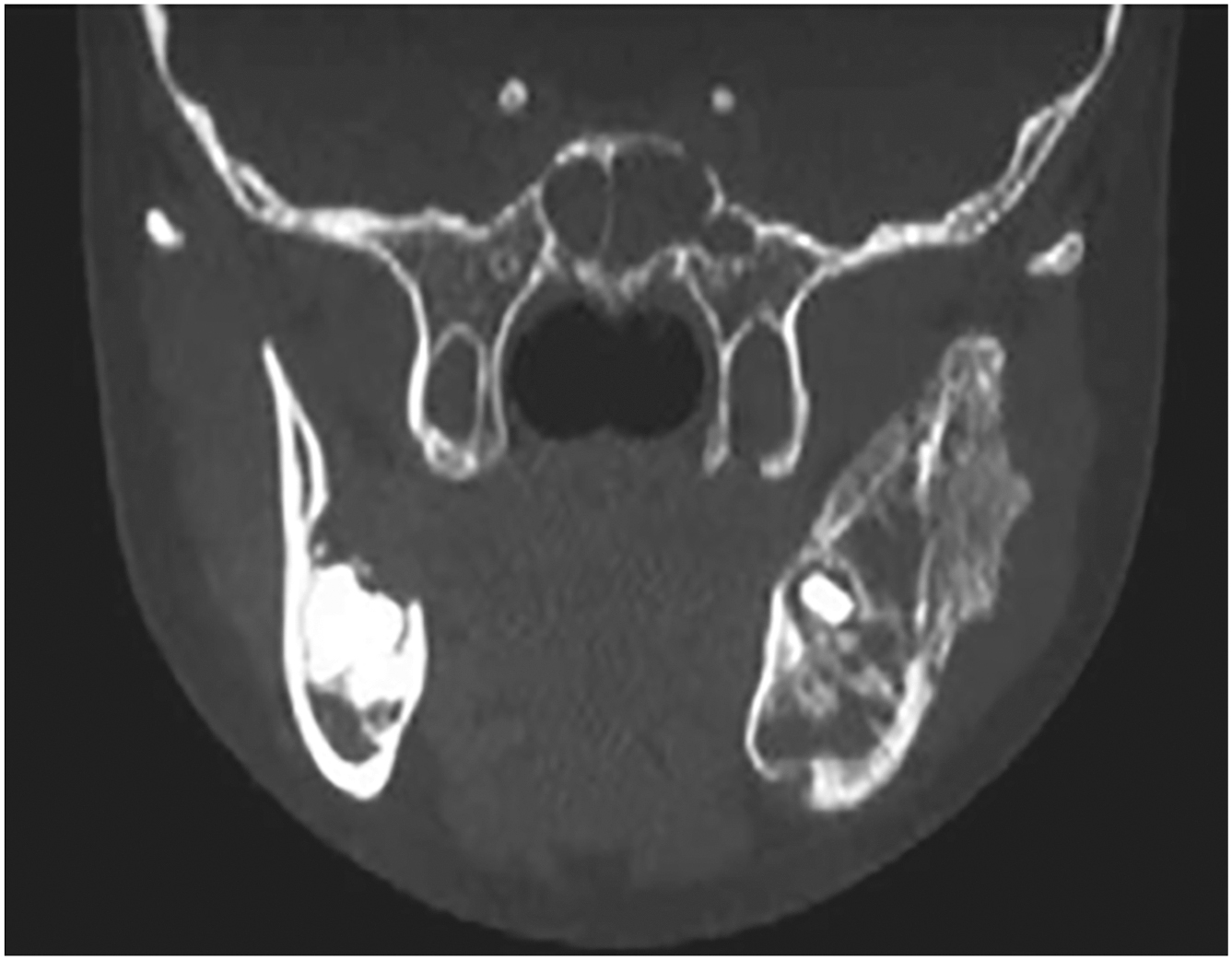
We present two cases to highlight the potential for excellent aesthetic and functional outcomes in pediatric patients undergoing free tissue transfer. Case 1. A young boy underwent fibula free flap reconstruction following Isolated neuroblastoma ( Fig. 1 ) resection from the mandible via segmental mandibulectomy ( Fig. 2 ). Rib graft was used for condylar head reconstruction and fibula for mandibular bone with temporalis tendon suspension ( Fig. 3 ). 1 year postoperative outcome demonstrates excellent occlusion and mouth opening ( Fig. 4 ). Case 2. A young girl presented with a parapharyngeal space tumor ( Fig. 5 ) found to be rhabdomyosarcoma. She underwent a lip split mandibulotomy approach with resection of the parapharyngeal space rhabdomyosarcoma ( Figs. 6 and 7 ). A radial forearm free flap was used to cover the pharyngeal space defect ( Fig. 8 ). Post-operative 1 year outcome with excellent aesthetic outcome and mandibular opening ( Fig. 9 ).
Related posts:
 Contemporary Approaches to Head and Neck Reconstruction
Free Flap Reconstruction of the Oropharynx
Contemporary Approaches to Head and Neck Reconstruction
Free Flap Reconstruction of the Oropharynx
 Advances in Midface Reconstruction
Advances in Midface Reconstruction
 Minimizing Donor Site Morbidity and Innovations in Donor Site Management
Minimizing Donor Site Morbidity and Innovations in Donor Site Management
 Updates in Free Muscle Transfers for Smile Reanimation
Updates in Free Muscle Transfers for Smile Reanimation
 Dental Rehabilitation in Maxillomandibular Free Flap Reconstruction
Dental Rehabilitation in Maxillomandibular Free Flap Reconstruction
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


