Androgenetic alopecia is a common cause of hair loss in both men and women. The exact pathogenesis of androgenetic alopecia is not well understood. As the name implies, the role of androgens and genetic susceptibility predisposes to pattern hair loss due to gradual conversion of terminal hair into vellus hair. Male and female pattern hair loss are clinically distinct entities but histologically indistinguishable. The role of sex hormones in females is less understood. This article discusses current understanding of the etiopathogenesis of hair loss in men, diagnostic tests available, and its medical management.
- •
Male pattern hair loss is common cause of hair loss in men.
- •
Androgens and genetic susceptibility predispose to pattern hair loss.
- •
Diagnosis is mainly by clinical examination.
- •
The screening test HairDX is available to diagnose susceptible individuals.
Introduction
Male pattern hair loss (MPHL) is the most common cause of hair loss in men. The incidence of pattern hair loss in men varies from population to population based on genetic background. The highest prevalence is reported in the Caucasian population. In the Asian population the frequency is lower than in Europeans. There is no information on the prevalence in African men.
Hair is an important feature of self-image. Studies have shown men who suffer from MPHL are 75% less confident, especially when interacting with the opposite sex. Young men with hair loss have reported loss of self esteem, introversion, and feeling unattractive to a higher degree than older men with hair loss. Although there is a significant impairment in quality of life in many patients, Alfonso and colleagues revealed that 3 out of 4 men with MPHL had never pursued therapy for hair loss. Men who seek medical help and are successfully treated reported psychological benefits with improvements in self esteem and personal attractiveness. By increasing the level of the patient’s knowledge about MPHL, early diagnosis and management can significantly reduce the psychological burden associated with this disease.
Pathophysiology
MPHL occurs in the presence of androgens in genetically susceptible individuals. The disease onset and progression vary from person to person. Initial signs of MPHL usually develop during teenage years, leading to progressive hair loss with pattern distribution. Bitemporal hair loss starts at the anterior hair line, resulting in a receding hair line followed by hair loss over the vertex and mid-frontal areas, with sparing of the occipital scalp.
Role of Androgen
Locally and systemically derived testosterone either directly binds to the intracellular androgen receptors mainly expressed within the dermal papilla and the hair bulb, or is metabolized into the more potent dihydrotestosterone (DHT) which, in turn, binds to androgen receptors with an approximately 5-fold greater affinity. The conversion of testosterone to DHT in the hair follicle is predominantly mediated by the 5α-reductase (type 1 and 2). It is thought that DHT is the key androgen required for the induction of MPHL. Changes in several factors along the androgen signaling pathway possibly lead to hair-follicle miniaturization, including an increase in the expression of androgen receptors, increased androgen sensitivity to bind more steroid ligand, and higher levels of 5α-reductase. The scalp has a combination of androgen-sensitive and androgen-independent hair follicles. Androgen-sensitive hair follicles are located on the frontal scalp and vertex whereas androgen-independent hair follicles are present on the sides and back of the scalp. This distribution of androgen receptors explains the clinical presentation of pattern hair loss. The success of hair transplantation is based on the fact that hair follicles harvested from the occipital scalp retain their androgen-independent behavior when implanted in the frontal scalp (donor dominance). Dermis of the frontoparietal scalp is derived from the neural crest, whereas dermis of the occipital and temporal scalp is derived from mesoderm. This difference in embryonic origin may explain the differential influence of androgens.
Role of Genetics
A polygenic mode of inheritance has been well established in MPHL. These genes may determine the age of onset, progression, patterning, and severity. Hypermethylation of DNA in gene promoter regions blocks the gene transcription machinery and therefore switches off gene expression, whereas hypomethylated gene promoters engage with gene transcription machinery to switch on gene expression. Partial demethylation of promoters that arises stochastically with age and with the effects of the environment leads to subtle changes in gene expression that are heritable. In balding scalp, differences in androgen receptor gene (AR) sensitivity and expression between vertex and occipital regions may be accounted for by the differential AR methylation patterns, leading to region-specific susceptibility to hair-follicle miniaturization.
The first published genetic link with MPHL was the discovery of a marked association with a particular single-nucleotide polymorphism (SNP) in exon 1 of the AR. This SNP is present in almost 100% of young and older balding men, but is also found in a significant proportion of older men unaffected by baldness, suggesting that this SNP is essential, but not sufficient, for MPHL in men. Genetic testing for MPHL is currently based on genotyping of the nonfunctional SNP in exon 1 of the AR that has been repeatedly associated with MPHL. The AR gene is located on the X chromosome, and men inherit it from their mother. This finding therefore confirms there is a maternal influence on male balding but does not explain the genetic contribution from the father. The identification of new susceptibility genes on chromosomes 3q26 and 20p11 suggest an androgen-independent pathway that is yet to be identified.
The difference in clinical presentation in men and women with pattern hair loss may be due to the following observations:
- •
Females have 3 to 3.5 times less 5α-reductase (types 1 and 2) than men.
- •
The enzyme cytochrome P450 aromatase converts testosterone into estradiol and estrone, which reduces conversion of testosterone into DHT. The aromatase level is significantly higher in the hair follicles of women and also 6 times more in the frontal follicles and 4 times more in the occipital hair follicles, which may explain why women usually retain their frontal hairline in contrast to men with pattern hair loss.
- •
Both men and women have 30% higher AR levels in the frontal hair follicles compared with occipital follicles, but the total receptor level is 40% less in women than in men.
Hair-Cycle Dynamics
The key feature in MPHL is follicular miniaturization. The hair cycle has an anagen phase or active growth phase lasting 3 to 5 years, catagen phase or transition phase lasting 1 to 2 weeks, and the telogen or resting phase lasting for 5 to 6 weeks. MPHL results from altered hair-follicle cycling and miniaturization, which leads to the transformation of terminal to vellus hair follicles. A reduction in anagen duration leads to shorter hair length, whereas an increase in telogen duration delays regeneration. This process results in hairs so short and fine that they fail to achieve sufficient length to reach the surface of the scalp, resulting in an increased number of empty pores and a reduction of anagen to telogen ratio. Small hair follicles result in finer hairs. The caliber of the terminal hair shaft is greater than 60 μm, the vellus hair measures less than 30 μm, and the thickness of indeterminate hair is between these two. The exact mechanism of follicular miniaturization remains unknown. The dermal papilla determines the size of the hair bulb and the hair shaft produced; it is likely the target of androgen-mediated events leading to miniaturizations and hair-cycle changes.
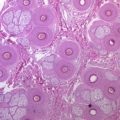
Histopathology
The characteristic histologic finding is an increase in number of vellus-like hair follicles or miniaturization ( Figs. 1 and 2 ).