Abstract
Most faces are asymmetrical, with asymmetrical bone structure and therefore overlying muscle volume. The art is to see the difference in sizes and actions of the muscle groups to predict possible difference in innervation of bilateral muscles once the botulinum toxin has blocked the nerve conduction to the muscle. For example, BOTOX will paralyse the frown muscle on one side more than the other if that side has a smaller glabellar complex. Treatment could divert the difference in muscle signalling to the other side, causing unwanted brow shapes. The art is to examine the patient first to predict the likelihood of certain muscles overacting, avoiding unwanted complications. Learning how to use BOTOX and Dysport to ‘neuromodulate’ is a powerful tool for managing facial asymmetry following facial palsy. Learning how to maintain the baseline tone in the muscle complex, without paralysing it completely, is the key to creating a natural look with treatment.
Keywords
Neuromodulation, Botox, Dysport, Xeomin, asymmetry, Symmetry, facial palsy, side effects, the art of Botox
One of the most difficult things to do for a beginner with botulinum toxin (BTX) is to anticipate how the other muscles on the face will react if injections are given to a muscle. It is easy to see what happens when the treated muscle is paralysed but less easy to anticipate where the signal to ‘that’ muscle will now divert to.
It is also tempting to assume that a right and left muscle will require the same dose for the same amount of paralysis, but because of natural asymmetry, this does not always happen.
The art lies in learning how to predict where the signals will go after treatment and how to anticipate and prevent unwanted action of other muscles on the face.
It is important to have a deep understanding of this signalling to muscles of the face before interfering with the muscle tone of a patient’s face and neck. Examples of muscle signal pairs are shown in Table 5.1 .
- ■
Think of BTX as blocking the innervation of a specific area of muscle, as opposed to blocking the whole muscle.
- ■
Always try to guess where the innervation will go to instead, once you have blocked it, and anticipate extra movement elsewhere which might need treatment.
- ■
Always remember the long-term effects you are creating via central control of innervation and feedback; this how you ‘train’ the muscles.
Never assume that both sides of the face receive equal innervation.
| Muscle Action | Paired Muscle Action |
|---|---|
| Corrugator | Depressor anguli oris (sad) |
| Frontalis muscle | Mentalis (horror) |
| Frontalis muscle | Depressor anguli oris |
| Frontalis muscle | Orbicularis oculi |
| Frontalis muscle | Zygomaticus |
| Orbicularis oculi | Zygomaticus (smile) |
Resting tone
The muscles of the face tend to mirror each other.
Many wrongly forget that the muscles have a resting tone when not contracting and assume that the muscles are relaxed when the patient is not actively contracting them. A good way to demonstrate what the patient will look like after resting tone is turned off is to examine their eyebrows. When the brows are gently massaged downwards, with the patient’s eyes shut, they often descend to a lower resting position. This is without resting tone. This is where they would ‘live’ if all their frontalis received BTX.
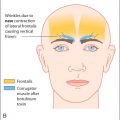
The basic nerve signal to a muscle of facial expression is usually from a tonically active neuron that is a cholinergic neuron that fires at 0.5 to 3 impulses per second during the entire duration of the stimulus. This allows the muscle to have a resting tone and to provide a baseline support to the facial structures in between voluntary facial movements. For example, the frontalis muscle of the forehead, innervated by the zygomaticofacial branch of the facial nerve VII, usually has a resting tone ( Fig. 5.1 A). The patient may raise the eyebrows on command by contracting the frontalis muscle (see Fig. 5.1 B), but it is usually possible to ‘relax’ the resting tone and to bring the brows to a lower level than their normal resting tone (see Fig. 5.1 C). This latter position imitates and thus demonstrates the unwanted result of too much BTX across the forehead in an unsuitable patient.