Abstract
The main serotypes of botulinum toxin comprise different concentration measurements. Each must be reconstituted specifically for its own brand, and doses must not be interchanged. However, BOTOX and Xeomin have been prepared from the same concentration system, and dilutions and dosages in the authors experience are very similar. Dysport and Azzalure derive from a different system. The author stresses that intuitive treatment of a muscle group of a patient, being mindful of neuromodulation, is well served by engaging the sense of ‘touch’. Pressure on the syringe equates to the volume dispelled and the area of tissue injected. The skill to equate volume with area of treatment may be honed with practice and exercises, beginning with a baseline concentration and adjusting only volumes. Unwanted side effects, such as ptosis, are extremely rare when the area of diffusion is known and the centre of injection is chosen an adequate distance from the muscle the injector is avoiding. Furthermore, expression can be shaped by utilising the action of the untreated muscle fibres in combination with the paralysed treated fibres (e.g. with brow lifts). Patient comfort may be optimised by learning how to penetrate the skin and muscle gently at 90 degrees where indicated, minimising the distortion of surrounding nociceptors.
Keywords
Side effects, diffusion, concentration, Dysport, Azzalure, Botox, Xeomin, skills training, pain.
NEVER handle botulinum toxin without surgical gloves.
Presentation
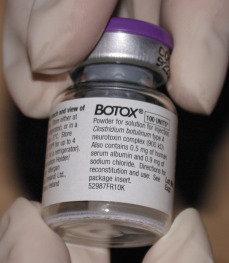
Botulinumtoxin A (BTX-A) vials have changed in size and shape over time. Specific instructions are readily available on the product websites and in the product insert packaging. Research is ongoing on the new liquid form of BTX-A, as well as topically applied preparations, but the three BTX-A products used by the author, onabotulinumtoxin A (onaBTX-A), incobotulinumtoxin A (incoBTX-A) and abobotulinumtoxin B (aboBTX-B), are presented as freeze-dried powder in a glass vial. The vials frequently look empty to the inexperienced eye because the powder tends to rest in their bottom angle ( Fig. 4.1 ). The vials vary in size, depending on brand and quantity of units, and this will influence the capacity for filling with normal saline for more dilute preparations.
There are strict guidelines for storage of botulinum toxin to prevent denaturation and maintain maximum efficacy. OnaBTX-A and aboBTX-A should be stored, before reconstitution, either frozen at −5°C or in a refrigerator at 2°C to 8°C until reconstituted. IncoBTX-A may be stored at room temperature, up to 25°C, until reconstituted. Once reconstituted, they all must be stored at 2°C to 8°C (refrigeration temperature). A thermos flask or a vaccination transporter may be used to maintain the solution at 2°C to 8°C if a refrigerator is not available in the clinic.
Reconstitution
It is recommended that all products are reconstituted with preservative-free normal saline, which is what the author routinely uses. Several studies have shown successful reconstitution with preserved normal saline, with reports of 48% more comfort when compared with preservative-free saline. Some studies have included 0.5% xylocaine to improve comfort.
The rubber seal on the vial should be wiped with an alcohol swab before using a 5-mL syringe to inject the desired volume of normal preservative-free saline. A green 25-gauge needle is inserted carefully through the centre of the bung, but care must be taken with BOTOX bungs, which can freeze solid. The needle can easily enter at an angle, releasing pieces of rubber into the solution.
Never agitate botulinum toxin solution when reconstituting it. It will not work!
The product is vacuum-sealed. If no pull on the plunger is felt, then the vial must be discarded. Air can be injected into the vial to avoid too rapid a reconstitution, and a thumb can be placed under the plunger of the syringe to control the rate of release of saline onto the powder ( Fig. 4.2 ). The saline must not gush in and agitate the solution mechanically. This will denature it by disrupting the delicate disulphide bonds. Studies have confirmed that it will still be effective but with a curtailed duration of effect. Rotating the vial during injection, and gently swirling the solution, will capture any powder trapped in the ‘lid’ part of the vials, especially with incoBTX-A (Xeomin/Bocouture).

Injection
We recommend using no bigger than 1 mL tuberculin or insulin syringes. These are essential for the dose to be gauged accurately during injection. The doses recommended in this book are given in units of volume. The finest mark on a 1-mL syringe is 0.01: we often recommend using 0.025 mL and 0.01 mL (more later). Beginners may prefer a 0.05-mL syringe. Constant practice with 0.5-mL insulin syringes and then 1-mL syringes ( Fig. 4.3 ) will develop the sense of touch to repeatedly administer small ‘droplets’ if necessary. The author prefers to use a 1-mL syringe and often more than one 30-gauge needle to keep the needle sharp while minimising stimulation of the nociceptors on the skin surface.

Always watch the gauge of the syringe while injecting to be certain of the volume you are injecting.
Aspiration
Always use gloves for self-protection. The solution should be aspirated freshly for each patient, although some doctors recommend preaspiration of BTX-A in several 1-mL syringes, and then storing them in the refrigerator. Manufacturers recommend a single vial per patient, which must be used within 4 hours of reconstitution.
Botulinum toxin is potent and very expensive, so each drop must be used to its maximum effect. Even an injection as small as 0.01 mL is effective in certain sites.
Take care to remove the 25-gauge needle from the bottle after aspiration, particularly with Dysport, where the combination of a small vial and a viscous solution encourages seepages from the needle.
Once aspiration is complete, attach a 30-gauge needle to the hub of the syringe. Take care that the batches of needles and syringes fit well together, and beware of attachments so loose that the toxin dribbles from the hub during injection. This is wasteful and may be hazardous if the leaked fluid contacts the patient’s face (ingestion of botulinum toxin droplets has been suspected of causing mild gastroenteritis). Clear the air bubble from the syringe using minimal agitation. This requires more care with Dysport/Azzalure because of its greater viscosity.
Wipe away any spilled botulinum toxin with a hypochlorite solution
Skill must be acquired to confidently be able to administer the lowest number of BTX units at the highest concentration (i.e. a very small volume of solution) repeatedly and accurately. It is easy to administer a dilute solution of the same units at a larger volume.
Injection technique
Good injection technique is critical for such a powerful agent because it takes a trained light touch to inject a tiny dose. Very few chemicals continue to be effective at such high dilutions. There is a real art to being able to manipulate the combination of extremely low with normal and high doses in the one treatment. The injections for rejuvenation are being administered to a continuum of facial muscle fibres. To be confident of offering aesthetically optimal treatment, the user must be skilled with injection technique. Once a single muscle tone is altered with a primary BTX-A injection, there is an immediate adaptation by both surrounding muscles, as well as remote ‘paired’ and contralateral muscles. Very small doses are excellent at controlling the secondary BTX-A effect. The user must be adept at injecting intradermally, subcutaneously, intramuscularly, giving small and large doses and, most of all, observing and avoiding arteries, veins and nerves.
The injector must know how to gauge the journey of the needle through the skin and muscle at different sites on the face and neck. This is a sense of touch which can be acquired only with practice.
Skill development
Practise:
- 1.
Entering the skin to create the least amount of pain
- 2.
Entering the skin and muscle to the correct depth
- 3.
Delivering the expected ‘circle of diffusion’ of toxin per volume injected.
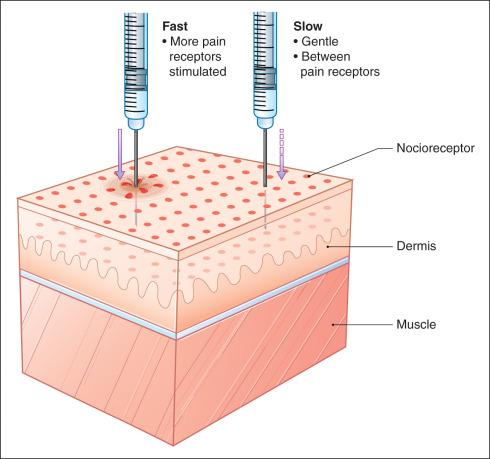
Pain
Topical anaesthesia makes little difference to the pain of intramuscular injections, unless highly concentrated (e.g. LMX) or in place long enough to penetrate. SLOW insertion of the needle makes a big difference to the perception of pain. The goal is to enter the skin without causing it to ‘dip’ and stimulate the pain receptors on either side ( Fig. 4.4 ). It helps to enter at a 90 degree angle to the surface because that is the smallest surface area stimulated. With practice, it is actually possible to ‘get lucky’, to enter in between the pain receptors with the patient feeling nothing.