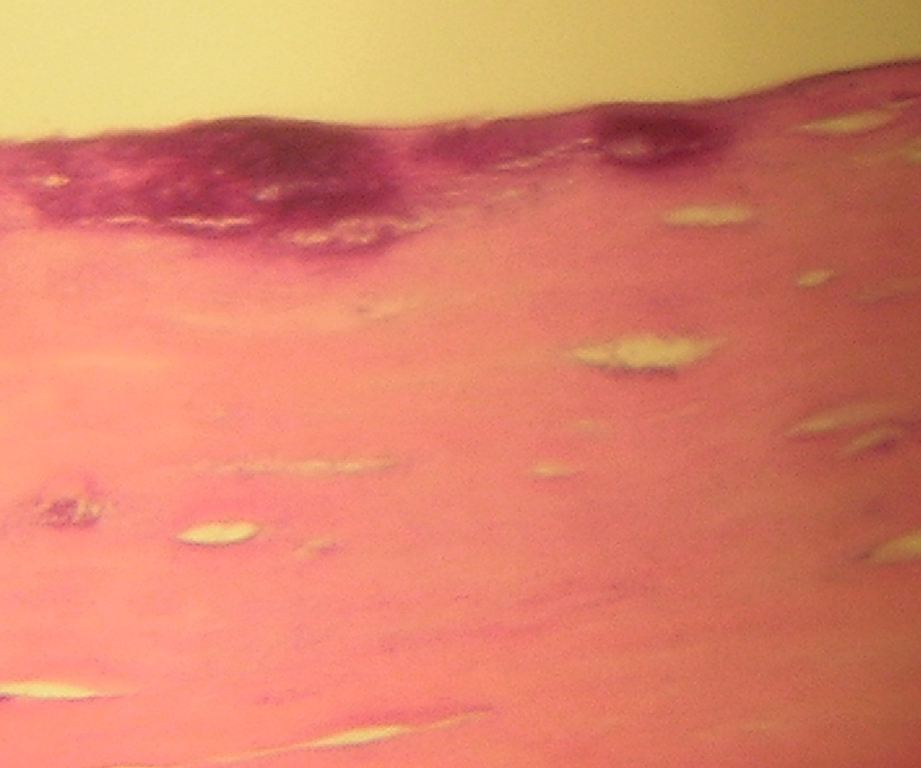
Capsule consisting of a sclero-hyaline tissue with a flat inner lining (35×)
Fig. 16.2
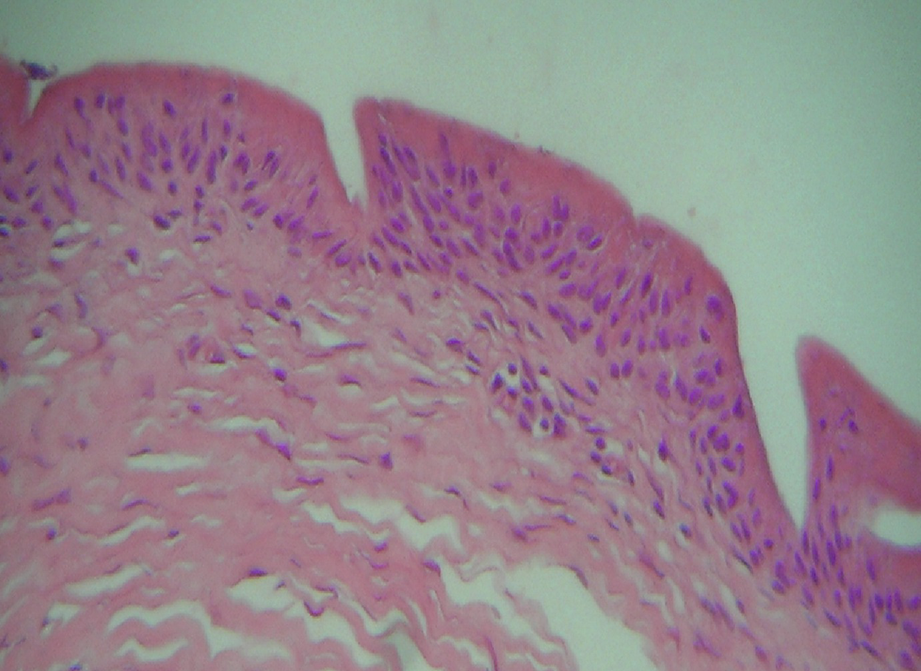
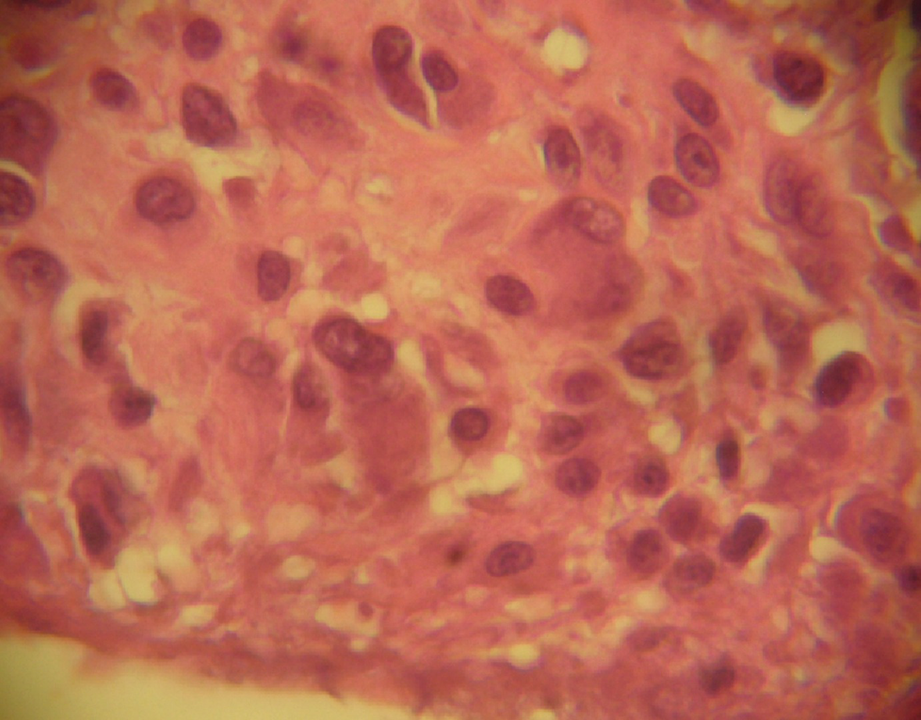
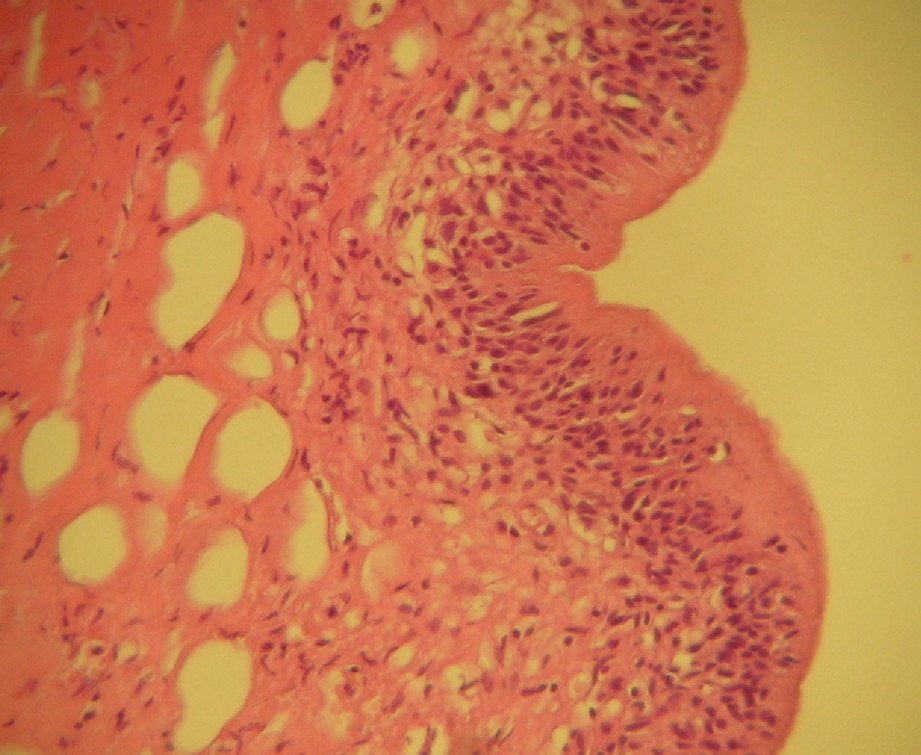
Internal surface of the capsule with a synovial lining (200×)
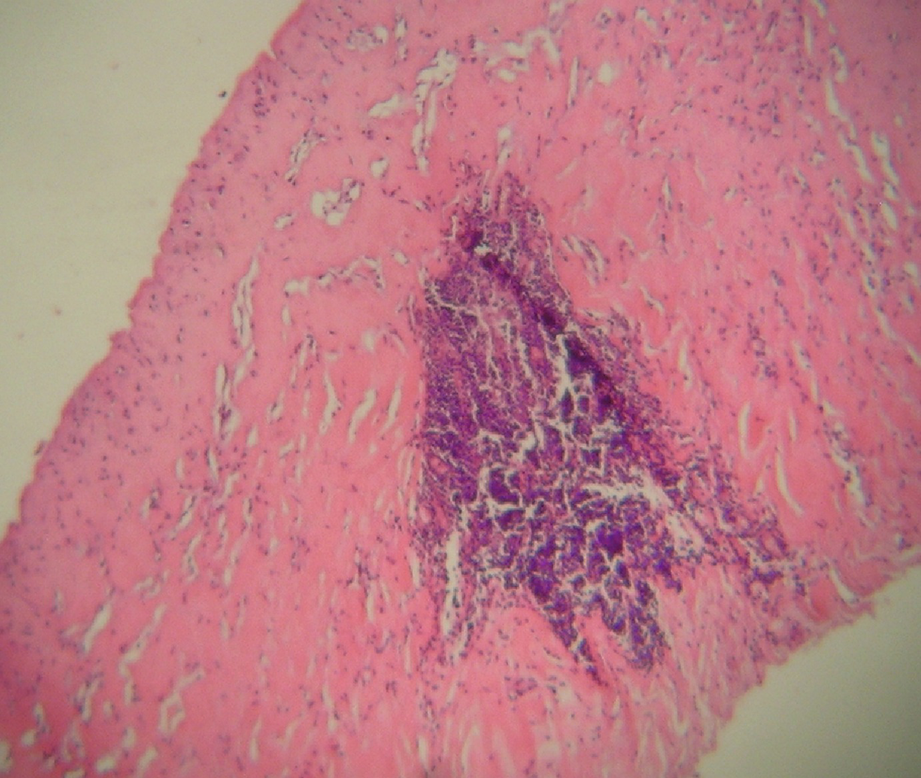
Synovial lining cells also have alpha 1 anti-chymotrypsin, lysozyme, and CD-48. By electron microscopy, their ultrastructure is similar to that of articular synovial cells [4]. It has been suggested that synovial metaplasia should be more common with prostheses that have a rough and textured surface than with prostheses with a smooth surface. This would be due to friction between the external surface of the prosthesis and the connective tissue of the inner surface of the periprosthetic capsule [5, 6]. In some cases, fibrin deposits (Fig. 16.3) and granulation tissue with numerous histiocytes are observed, along with giant cells on the internal capsular surface. Multinucleated cells may appear, with the progressive transformation of granulation tissue histiocytes into synoviocytes (Figs. 16.4, 16.5, 16.6). The synovial lining may, eventually, mimic papillary hyperplasia, forming papillae on its surface that, with a small biopsy, may be confused with a papillary lesion of mammary glandular tissue.
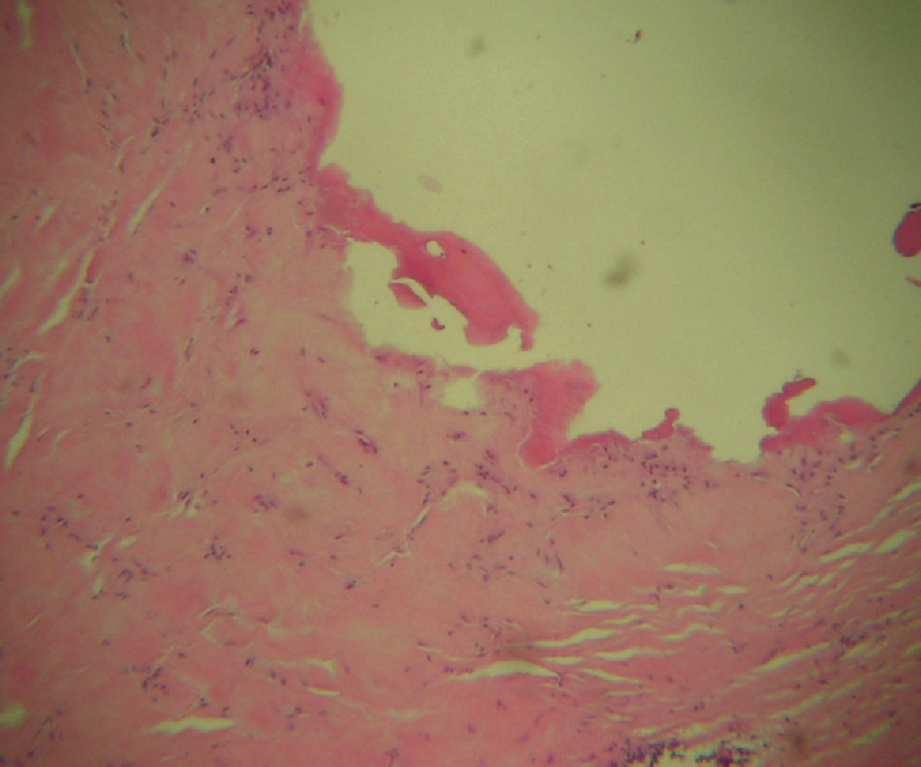
Fig. 16.3
Deposit of fibrinoid material on the inner surface of the capsule (100×)
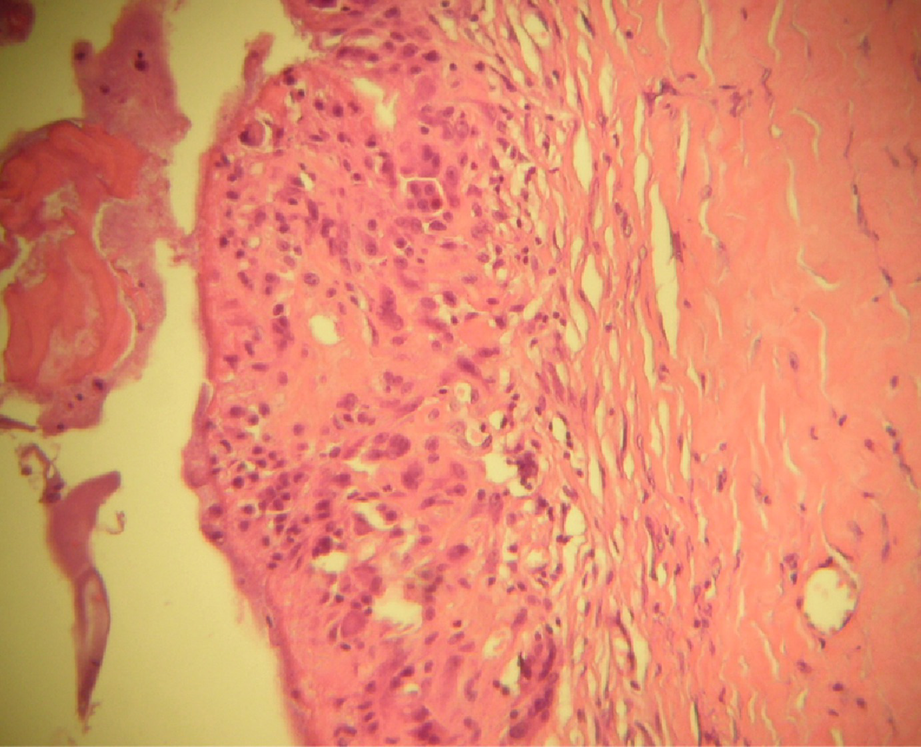
Fig. 16.4
Internal surface of the capsule with deposits of fibrinoid material and histiocytes that becomes synoviocytes (200×)
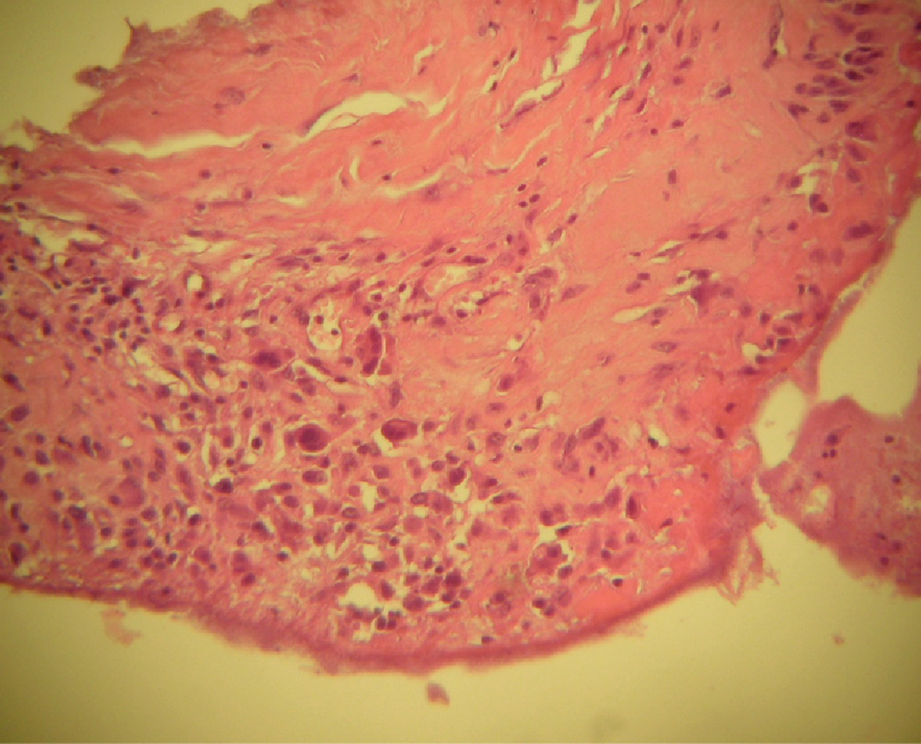
Fig. 16.5
Similar appearance upon magnification; note the multinucleated giant cells (200×)
Fig. 16.6
Similar appearance upon further magnification (350×)
Within the connective layer, a variable degree of lymphocytic infiltration can be observed (Fig. 16.7); in some cases, this lymphocytic infiltration is marked, largely composed of T lymphocytes [7, 8] that, immunohistochemically, are predominately positive for CDH, CD29, and HLA-DR; this suggests an immunological response to the prosthesis [9]. The lymphocytic infiltration is accompanied by increased local tissue concentrations of hyaluronic acid and interleukin-2 (IL-2) [10]. Occasionally, in cases of marked lymphocyte infiltration is necessary to perform immunohistochemical techniques to confirm the reactive nature of the lymphocytic infiltrate and rule out a lymphoproliferative process, since CD30 positive lymphomas, have been described in association with periprosthetic capsules [11, 12].
Fig. 16.7
Capsule consisting of sclero-hyaline tissue, with lymphocytic infiltration (200×)
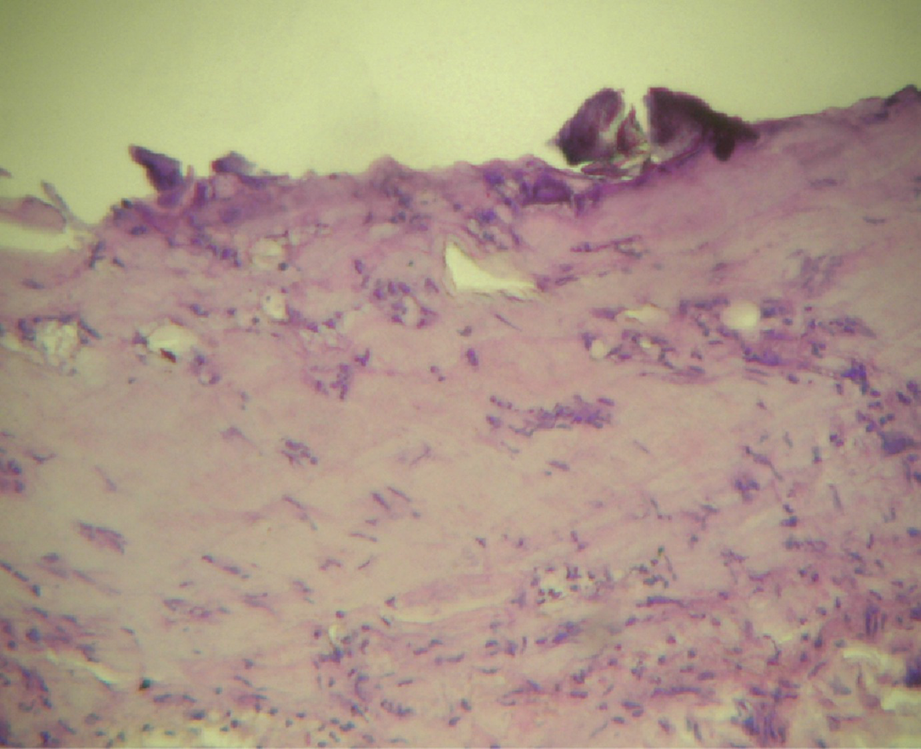
In old capsules, there is an increasing fibrosis, hyalinization, and calcium deposits (Fig. 16.8), which can vary between small foci and thick calcifications, both on the internal surface of the capsule (Fig. 16.9) and throughout its thickness. These alterations are usually observed in old capsules that have been extracted during prosthesis-replacement procedures, even without prosthesis rupture or the formation of the so-called siliconomas. The presence of calcified foci is related to the age of the prosthesis [13].
Fig. 16.8
Sclero-hyaline capsule with areas of calcification (300×)
Fig. 16.9
Sclero-hyaline capsule with calcified lumps on the inner surface (300×)
Small lumps of prosthetic material (Fig. 16.10), corresponding to siliconomas, are frequently observed within the connective tissue layer, even when the prosthesis appears grossly intact. This material can be observed in hematoxylin-eosin stained sections, but it becomes more evident when the microscope’s condenser is closed to reduce illumination, even without using polarized light or other special techniques. This finding of small particles within the thickness of the periprosthetic capsule, in an intact prosthesis, can be explained by the filtration of prosthesis material through the prosthesis wall. Van Diest et al. [14] have classified the degree of silicone filtration through the capsule into four stages: (1) no infiltration, (2) evidence of silicone particles in the inner half of the capsule, (3) infiltration reaching the outer half of the capsule, and (4) transparietal infiltration. These stages correlate with the implant’s age. The filtration of silicones is related, on one hand, to an autoimmune reaction, and, on the other, to the migration of prosthesis material through tissues, even to sites outside the breast, like regional or even distant lymph nodes [15–17].
Fig. 16.10
Sclero-hyaline capsule with silicone lumps within the thickness of the wall and internal surface, with a synovial lining (200×)
Only gold members can continue reading. Log In or Register to continue